
Alcoholism in India- Concerns, Challenges and Way Forward
From Current Affairs Notes for UPSC » Editorials & In-depths » This topic
In March, India, like several countries shut down liquor shops. During this period, the mental health of many alcoholics deteriorated with several even attempting suicides. When the shops were reopened in May, long queues and chaotic crowds with blatant disregard for social distancing norms were observed across the country. States have started online sale of liquor. This calls for a look into the issue of alcoholism in India.

This topic of “Alcoholism in India- Concerns, Challenges and Way Forward” is important from the perspective of the UPSC IAS Examination , which falls under General Studies Portion.
Why is alcoholism a cause of concern?
- Alcohol, by its nature, is toxic and has ‘dependence inducing properties’ .
- It causes about 3 million deaths across the world every year, according to Global Status Report on Alcohol and Health, 2018 , released by WHO .
- Globally, it is responsible for 1% of disease burden . Alcohol is responsible for disease burden more among males (7.1%) than females (2.2%) . This alcohol-attributable disease burden is especially high in low income and lower middle income countries .
- It is a leading risk factor for premature deaths and disabilities in the 15-49 years age group. 10% of all deaths in this age group can be attributed to alcohol consumption.
- Most of the alcohol related deaths among males were due to injuries , digestive diseases and alcohol use disorders (AUD) . In case of females, it was mainly due to cardiovascular diseases , digestive diseases and injuries .
- Alcohol related hospitalization and deaths is higher among the vulnerable and disadvantaged
- The harmful use of alcohol has a direct impact on the countries’ progress towards Sustainable Development Goals – especially with regards to the health related targets like child and maternal health , infectious diseases like TB and AIDS , non-communicable diseases, mental health , poisoning, etc. Annual per capita consumption of alcohol is an indicator for target 3.5 of SDG i.e. “Strengthen the prevention and treatment of substance abuse, including narcotic drug abuse and harmful use of alcohol”.
- Alcoholism cements the inequalities between countries with the poorer countries facing higher ‘harm per litre’.
In times of COVID-19
- There has been a world-wide increase in domestic abuse cases with people staying indoors with their families for longer periods. WHO opines that alcohol can be a contributing factor.
- In the initial periods of the COVID-19 outbreak, rumours about alcohol killing off the virus led to deleterious effects. In fact, ethanol consumption is known to weaken the immune system .
- 700 people were killed in April in Iran when they consumed methanol believing that it might cure the disease . This is despite Iran being a prohibition country.
- During the initial stages of lockdown, suicides were one of the leading causes of death. Alcohol withdrawal was identified to be one of the reasons.
- People have been drinking more alcohol to overcome the boredom due to the lockdown .
Express Learning Programme (ELP)
- Optional Notes
- Study Hacks
- Prelims Sureshots (Repeated Topic Compilations)
- Current Affairs (Newsbits, Editorials & In-depths)
- Ancient Indian History
- Medieval Indian History
- Modern Indian History
- Post-Independence Indian History
- World History
- Art & Culture
- Geography (World & Indian)
- Indian Society & Social Justice
- Indian Polity
- International Relations
- Indian Economy
- Environment
- Agriculture
- Internal Security
- Disasters & its Management
- General Science – Biology
- General Studies (GS) 4 – Ethics
- Syllabus-wise learning
- Political Science
- Anthropology
- Public Administration
SIGN UP NOW
How prevalent is alcoholism in India?
- India is one of the largest consumers of alcohol in the world. Of all alcohols, India is the 9 th largest consumer by volume .
- After China , it is the largest consumer of spirits – especially of whisky . Almost one in every two bottles of whisky brought in the world is sold in India. During the 2018 global dip in alcohol consumption, India was instrumental in driving a 7% uptick in the global whisky sales.
- There has been an 11% increase in consumption since 2017 – i.e. consuming over 663 million litres .
- The per capita consumption of alcohol is also increasing.
- Highest prevalence is in Chhattisgarh, Tripura, Punjab, Arunachal Pradesh and Goa .
- Over 45% of all the liquor sold in India is in just 5 southern states : Andhra Pradesh, Telangana, Tamil Nadu, Karnataka and Kerala . Notably, over 10% of these states’ revenues is from taxes on liquor sales.
- The next largest consumers in India are Punjab, Rajasthan, Uttar Pradesh, Madhya Pradesh, West Bengal and Maharashtra .
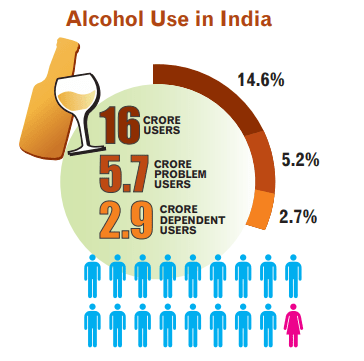
- According to the 2019 Magnitude of Substance Use in India report from the social justice ministry, alcohol is the most common psychoactive substance used by Indians.
- Over 14% of the 10-75 years age group consume alcohol. This means that 16 crore people consume alcohol.
- Predominantly consumed alcoholic beverages in India are ‘desi sharab’ (country liquor) and spirits (Indian made Foreign Liquor) – each accounting for 30% .
- AUD is prevalent in the states of Tripura, Andhra Pradesh, Punjab, Chhattisgarh and Arunachal Pradesh . An additional 5% of the population consume alcohol in a harmful way .
- The report highlighted that 1 in 5 alcohol users are affected by alcohol dependence and hence require urgent treatment .
- 11% of Indians are binge drinkers according to WHO. This is against a global average of 16% .
- A major cause of concern is that more than half of alcohol consumed in the country is ‘unrecorded alcohol’ according to WHO. 1/3 rd of consumers drink cheap local brews – often adulterated and resulting in tragedies .
- A 2014 survey by International Alliance of Responsible Drinking found a preference for such local or homemade brews among a large number of drinkers.
Prelims Sureshots – Most Probable Topics for UPSC Prelims
A Compilation of the Most Probable Topics for UPSC Prelims, including Schemes, Freedom Fighters, Judgments, Acts, National Parks, Government Agencies, Space Missions, and more. Get a guaranteed 120+ marks!
Why does India have high levels of alcohol consumption?
- One of the reasons for the increase in alcohol consumption in India is that more people are earning sufficient income to purchase it. This has outpaced the efforts to reduce consumption.
- Alcohol is becoming increasingly affordable . This trend is also observed in low and middle income countries worldwide- more than in high income countries.
- Increased urbanisation and an expanding middle class are also contributors.
- Social pressures are a major contributor to the high prevalence of alcohol consumption in India. Many social activities are centred on alcohol and the drink being perceived as a ‘social lubricant’ .
- A 2019 survey noted the increased consumption of alcohol among women – referred to as ‘the pinking’ of the alcohol market- as a contributor too.
- Political dependence on the revenue generated by the industry- especially among the states. This was evidenced by how states decided to reopen liquor shops despite a fast growing pandemic to improve their revenues.
- Sustained messaging about the ‘attractions of alcohol consumption’ via movies and other TV programs .
- Aggressive marketing by the alcohol industry.
- Lax regulation of the industry.
- Low awareness about the negative impacts of alcohol on health.
What are the measures taken by government to reduce alcoholism in India?
- The Constitution itself has provisions for bringing in alcohol prohibition in India. Article 47 of the Directive Principles of State Policy states that “the State shall endeavour to bring about prohibition of the consumption except for medicinal purposes of intoxicating drinks and of drugs which are injurious to health”
- Several states have imposed prohibition on alcohol. These states, dubbed ‘the dry states’ , include Gujarat, Bihar, Manipur and Nagaland . Complete alcohol ban is also in force in the UT of Lakshadweep .
- States have imposed a legal drinking age in their jurisdiction. In some states it is 18 years , while in others it is 21 years and in yet others it is 25 years .
- Under the Motor Vehicles Act , any person found driving with a blood alcohol content of over 0.03% ( drunken driving ) is penalized. Punishment may even entail a prison term of up to 4 years .
- Advertisement of alcoholic beverages on television is banned in India.
- The Social Justice and Empowerment Ministry has been implementing the Scheme of Prevention of Alcoholism and Substance (Drug) Abuse since the 1980s . This scheme makes use of voluntary organizations (and others) to provide a range of services like identification, counselling, treatment, rehabilitation, creating awareness, etc. It targets a wide range of people with special focus on children, youth, women, prison inmates and other high risk groups like sex workers, drivers, etc.
- A toll-free helpline was set by the centre in 2015 to assist people with regards to substance dependence.
- In 2016 , the Supreme Court banned the sale of liquor within 500 m of any national or state highway . In 2004 , the National Road Safety Council too had agreed that liquor shops should not be licensed to open shop along national highways.
- The government has set a National Target to achieve a 10% reduction in prevalence of alcohol use by 2025 .
- Several state governments have permitted the online sale of alcohol to reduce aggregation of crowds at the liquor shops.
- Recently, on International Day Against Drug Abuse and Illicit Trafficking, the centre launched the ‘Nasha Mukt Bharat’ campaign to curb alcoholism and drug abuse in India. 272 districts identified as ‘vulnerable’ are to get treatment and de-addiction facilities .
- India has an international obligation to curb alcoholism as it is signatory to the UN Conventions- Convention on Psychotropic Substances, 1971 and Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances, 1988 .
What are the challenges?
- Imposition of prohibition is known to have several adverse unintended consequences as seen from the American Prohibition experiment from 1920 to 1933 . Its unintended consequences include the emergence of an entire black market for alcohol composed of speakeasies, bootleggers, organized crime syndicates , etc. which operated in every segment from production to distribution and sale. There was a significant increase in the number of deaths due to poisoning by methanol and other adulterants present in these illegally manufactured beverages.
- Strict regulations often have the unintended consequence of fuelling black market operations and consequently more dangerous versions of the banned product coming into the market.
- Several experiments with making alcohol more expensive only produced ‘small and modest’ reduction in its consumption.
- A huge part of state revenues is from sale of alcohol.
- There is a prevalence of nexus between the liquor barons and the political class .
- A day before the Supreme Court order regarding the ban of alcohol sales near highways, the rules were diluted to allow for several exemptions, after allegations of ‘judicial policymaking’ and several concerns raised about the livelihood of the alcohol industry’s stakeholders.
- The closing down of liquor shops in the initial periods of lockdown failed to reduce domestic abuse cases. Experts opined that alcohol is simply an excuse used by abusers to act violently against family members. Now, they use the lack of alcohol as an excuse to abuse.
- There was an increase in alcohol smuggling across the state borders and emergence of black markets .
- The reopening of liquor shops led to gross disregard for social distancing norms among the alcohol consumers.
- The lockdown increased consumption of alcohol. This is perceived as a result of people trying to overcome boredom apart from lack of work , isolation and stress arising from general uncertainty.
- In the current times, revenue shortages are faced by the states with the lockdown restricting normal economic activities. At the same time, governments have to provide for the basic food and social security of the people. Hence, there is very low incentive for the government to bring in any serious schemes to curb alcoholism.
- The online sale and home delivery of alcohol, if it becomes the new norms, will increase the availability of alcohol . This would be detrimental to the efforts to restrict its availability over the years.
What is the way forward?
- Reducing alcoholism cannot be achieved using a one-off method or a sudden blanket ban across the country. It needs to be brought in by phases .
- Political will is a key component in reducing the harmful use of alcohol.
- The policies designed for the purpose must be tailor made for local circumstances . It should be comprehensive and inclusive with clarity in division of responsibilities.
- A dedicated agency can be established for following up on the implementation of these policies and the consequent action plans and implementation mechanisms.
- The primary care physicians are the first point of contact for those suffering from AUD. This presents a valuable route of action in AUD control. These physicians can be equipped with tests like the WHO prescribed AUDIT (AUD Identification Test) to identify at-risk people and those with milder levels of AUD.
- They can be trained to manage problems using 3 core steps:
- One-on-one counselling to create awareness about ill effects of alcohol.
- Prescription of medications (eg: disulfiram ) in necessary cases.
- Referring patients to higher levels of care for treatment and rehabilitation.
- The health and social service providers for tackling AUDs must be made culturally sensitive . There is a need to de-stigmatize the issue to encourage more people to seek help and reduce relapses.
- The penalty for drunken driving must be appropriate enough to have a deterrent effect . Provision of alternate means of transport after the drinking hours can reduce alcohol-related accidents.
- The benefit of ‘behaviour change communication’ was seen with India’s Swachh Bharat Abhiyan . This could also be used for curbing problematic alcohol use.
- The WHO identified 10 key areas where the countries could focus on, with regards to interventions and policy options:
- Leadership, awareness and commitment
- Health services’ response
- Community action
- Drink-driving policies and countermeasures
- Availability of alcohol
- Marketing of alcoholic beverages
- Pricing policies
- Reducing the negative consequences of drinking and alcohol intoxication
- Reducing the public health impact of illicit alcohol and informally produced alcohol
- Monitoring and surveillance
As recent as in February, 2020, the WHO Executive Board unanimously identified global alcohol burden as a ‘public health priority’ . It called for ‘accelerated action’ to curb alcohol harm. Article 21 of the Constitution puts an obligation on the government to preserve the life of the people. Continued free availability of alcohol will have an especially adverse effect in the present times. Sustained and systematic efforts to largely eliminate harmful alcohol use in the society will have a major bearing on public health and the general quality of life.
Practice question for mains
Several state governments have opted for online sale of alcohol in the midst of a pandemic. Compare the pros and cons of this decision. (250 words)
https://www.who.int/health-topics/alcohol#tab=tab_1
https://apps.who.int/iris/bitstream/handle/10665/274603/9789241565639-eng.pdf?ua=1
https://www.newindianexpress.com/world/2020/apr/29/700-killed-in-iran-after-drinking-toxic-methanol-to-cure-coronavirus-2136857.html
https://www.bbc.com/news/world-asia-india-52640266
http://socialjustice.nic.in/writereaddata/UploadFile/Magnitude_Substance_Use_India_REPORT.pdf
https://timesofindia.indiatimes.com/india/womens-increased-alcohol-consumption-contributing-to-indias-growing-love-for-alcohol-survey/articleshow/70960088.cms
https://www.hindustantimes.com/india-news/pour-me-another-india-s-alcohol-intake-up-38/story-z8iVSto80HzG5A1RLl6HwN.html
https://vikaspedia.in/social-welfare/social-awareness/schemes/scheme-of-prevention-of-alcoholism-and-substance-drug-abuse-2015
https://thewire.in/government/liquor-sale-alcohol-coronavirus
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7014857/
https://timesofindia.indiatimes.com/india/centre-to-build-treatment-de-addiction-facilities-in-272-districts/articleshow/76648876.cms
https://www.business-standard.com/article/news-ians/toll-free-helpline-launched-for-alcohol-and-drug-addicts-115010700943_1.html
https://scroll.in/article/833499/supreme-court-explains-why-its-highway-liquor-shop-verdict-is-not-judicial-overreach
https://www.pbs.org/kenburns/prohibition/unintended-consequences/
GET MONTHLY COMPILATIONS
Related Posts

Quality in Pharma Sector- Lessons from Gambia Episode
GEMCOVAC-OM
There was a problem reporting this post.
Block Member?
Please confirm you want to block this member.
You will no longer be able to:
- See blocked member's posts
- Mention this member in posts
Please allow a few minutes for this process to complete.

Drug Abuse in India: Explained, pointwise
ForumIAS announcing GS Foundation Program for UPSC CSE 2025-26 from 19 April. Click Here for more information.
ForumIAS Answer Writing Focus Group (AWFG) for Mains 2024 commencing from 24th June 2024. The Entrance Test for the program will be held on 28th April 2024 at 9 AM. To know more about the program visit: https://forumias.com/blog/awfg2024
- 1 Introduction
- 2 What is the magnitude of drug abuse in India?
- 3 What are the impacts of drug abuse?
- 4 What are the challenges associated with drug abuse in India?
- 5 What are the government initiatives to tackle drug abuse in India?
- 6 What should be done to tackle drug abuse in India?
- 7 Conclusion:
Introduction
Recently, an investigation by Indian Express has revealed that a epidemic of drug addiction, mostly affecting young men, is sweeping across Kashmir. Drug abuse is a significant social and health issue in India. India’s diverse population, large youth demographic, and economic disparities contribute to the complex nature of drug abuse in the country. Changing cultural values, increasing economic stress and dwindling supportive bonds are leading to initiation into substance use.
What is the magnitude of drug abuse in India?
According to the Ministry of Social Justice and Empowerment’s report on the “ National Survey on Extent and Pattern of Substance Use in India ” (2019), the magnitude of substance use is:
- 16 crore people (14.6%) between the age of 10 and 75 years are current users of alcohol, and out of them, 5.2% are alcohol dependents.
- About 3.1 crore individuals (2.8%) are cannabis users, and 72 lakh (0.66%) people suffer from cannabis problems.
- Overall opioid users 2.06% and nearly 0.55% (60 lakh) require treatment services/health
- 18 crore (1.08%) are current users of sedatives (non-medical use).
- 7% of children and adolescents are inhalant users as compared to adults of 0.58%. Nearly 18 lakh children need help for inhalant use.
- It is estimated that about 8.5 lakh people are injecting drugs
The most worrying category of drugs in India are opioids , with the prevalence of opioid use in India being three times the global average (0.7% Vs 2.1%). Across all the drug categories, drugs in the opioid group (particularly heroin) are associated with the highest rates of disease, death and disability.
India’s location between the Golden Crescent (Iran-Afghanistan-Pakistan) and the Golden Triangle (Thailand-Laos-Myanmar) provides easy access to opioids.
The World Drug Report, 2022, ranked India fourth in terms of the quantity of seized opium in 2020, with a total of 5.2 tons confiscated. Additionally, India was ranked third for the amount of seized morphine in the same year, totaling 0.7 tons.
What are the impacts of drug abuse?
Health Consequences: Drug abuse can lead to a range of physical health problems, including liver disease (from alcohol), infectious diseases (due to sharing needles in injection drug use), and overdose-related deaths. Also, substance abuse is closely linked to mental health disorders such as depression and anxiety. It can exacerbate existing mental health issues or lead to the development of new ones.
Social and Family Impacts : Drug abuse can lead to family breakdowns, increased conflicts, and emotional trauma within families. Children in households affected by drug abuse may experience neglect, abuse, and disrupted education, affecting their overall well-being. Individuals struggling with drug addiction often face social stigma, which can hinder their recovery and reintegration into society.
Economic Consequences : Families often face financial hardships due to the costs of supporting a family member’s addiction and the associated medical expenses. With most drug users being in the productive age group of 18–35 years, drug addiction can lead to absenteeism and reduced productivity in the workplace.
Crime: An increase in violence and crime is the direct impact of drug abuse. Addicts resort to crime to pay for their drugs. Drugs remove inhibition and impair judgement, encouraging one to commit offences. The incidence of eve-teasing, group clashes, assault, and impulsive murders increases with drug abuse.
What are the challenges associated with drug abuse in India?
Lack of Awareness and Education : There is limited awareness about the risks of drug abuse and its consequences among the general population, particularly in rural areas. Also, educational programs in schools and communities to inform people, especially young individuals, about the dangers of drug abuse are insufficient.
Stigma and Discrimination : Stigmatization of individuals with substance use disorders can discourage them from seeking help and support. Discrimination in healthcare facilities and society at large can hinder access to treatment and rehabilitation services.
Limited Access to Treatment and Rehabilitation : There is a huge shortage of drug addiction treatment facilities and qualified healthcare professionals.
Inadequate Research and Data : There is limited research on the prevalence and patterns of drug abuse in India, which hampers evidence-based policymaking and program development. There are also challenges in collecting accurate data due to the hidden and stigmatized nature of drug abuse.
Easy availability of drugs: India’s geographic location close to major opium producing regions leads to easy availability of these drugs. Also, according to the Narcotics Control Bureau (NCB), there is a growing trend of using the ‘dark net’ and cryptocurrency for illicit drug trade.
New substances: The consumption of new psychoactive substances is increasing in India, and these substances often fall outside the scope of existing drug control regulations, posing challenges for law enforcement agencies to effectively monitor and regulate them.
What are the government initiatives to tackle drug abuse in India?
Laws: The broad legislative policy is contained in the three Central Acts, viz. Drugs and Cosmetics Act, 1940, The Narcotic Drugs and Psychotropic Substances Act, 1985, and The Prevention of Illicit Traffic in Narcotic Drugs and Psychotropic Substances Act, 1988.
Narcotics Control Bureau (NCB): It is the nodal agency for drug law enforcement in India. It was established in 1986 to coordinate drug law enforcement efforts across the country.
National Narcotics Coordination Portal : The multiplicity of stakeholders in Drug Law Enforcement has necessitated coordination between various agencies on real time basis. The Ministry of Home Affairs has constituted a four-tier coordination mechanism for increasing coordination amongst the nationwide stakeholders from grass root level to apex level and effectively combating the menace of drugs. The Apex NCORD, Executive NCORD, State NCORD and District CORD are four pillars of mechanism.
Integrated Rehabilitation Centers for Addicts (IRCAs): The Ministry of Social Justice and Empowerment (MoSJE) provides financial assistance to NGOs and voluntary organizations for the maintenance of Integrated Rehabilitation Centers for Addicts (IRCAs). These centers offer comprehensive rehabilitation services to individuals with substance abuse disorders.
National Action Plan for Drug Demand Reduction (NAPDDR): The MoSJE launched the NAPDDR for 2018-2025. The Plan aims at reduction of adverse consequences of drug abuse through a multi-pronged strategy.
Nasha Mukt Bharat Abhiyaan/Drugs-Free India Campaign : It was flagged off on 15th August 2020 (Independence Day) for 272 districts across 32 State/Union Territories that have been identified as the most vulnerable in terms of usage of drugs in the country. It is operational with the involvement of more than 500 voluntary organizations across the country, which are assisted financially under the NAPDDR scheme.
International Treaties: India is signatory to various international treaties and conventions to combat the menace of drug abuse like UN Convention on Narcotic Drugs (1961), UN Convention on Psychotropic Substances (1971), UN Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances (1988) and UN Convention against Transnational Organized Crime (UNTOC) 2000.
What should be done to tackle drug abuse in India?
Scientific evidence-based treatment needs to be made available at adequate scale for people with substance use disorders.
The government should take measures to strengthen the law enforcement agencies involved in drug control, including Customs, the Narcotics Control Bureau, and state police forces. This can include providing them with better training, technology, and resources.
Socio-economic factors like poverty, unemployment, and lack of education can contribute to drug abuse and trafficking. Therefore, the government can address these issues through poverty reduction measures, employment generation schemes, and increasing access to education.
Reducing demand for drugs can be done through community-based prevention programs, education, and awareness campaigns.
Conclusion:
Addressing drug abuse requires a holistic and multi-pronged approach that includes prevention, education, treatment, harm reduction, policy reforms, and increased community involvement. Collaboration between government agencies, healthcare providers, NGOs, and the community is essential to mitigate the impact of drug abuse in India.
Sources: Indian Express , MoSJE Report

Type your email…
Search Articles
Latest articles.
- Aayushi Bansal, UPSC IAS 2023 Topper, AIR 97 – Biography, State, Marksheet, and Answer Copy
- Rohit Tyagi, UPSC IAS 2023 Topper, AIR 74 – Biography, State, Marksheet, and Answer Copy
- UPSC Prelims Marathon 19th April – National Institutions and Environmental organization and National Missions on Environment – 2024
- 10 PM UPSC Current Affairs Quiz 18 April, 2024
- 9 PM UPSC Current Affairs Articles 18 April, 2024
- Increased tax collections in Northeast India: GST adoption gave north-eastern states a big developmental push
- Impact of Silicon Valley’s growth on local urban areas: Concrete jungles and Silicon Valleys
- Reasons for heavy rains in the UAE: What’s behind heavy rainfall in Dubai
- Supreme Court’s decision on the dispute between Delhi Metro (DMRC) and Delhi Airport Metro Express (DAMEPL)
- Just Transition Framework-A path to ecological justice
Prelims 2024 Current Affairs
- Art and Culture
- Indian Economy
- Science and Technology
- Environment & Ecology
- International Relations
- Polity & Nation
- Important Bills and Acts
- International Organizations
- Index, Reports and Summits
- Government Schemes and Programs
- Miscellaneous
- Species in news
Call us @ 08069405205

Search Here

- An Introduction to the CSE Exam
- Personality Test
- Annual Calendar by UPSC-2024
- Common Myths about the Exam
- About Insights IAS
- Our Mission, Vision & Values
- Director's Desk
- Meet Our Team
- Our Branches
- Careers at Insights IAS
- Daily Current Affairs+PIB Summary
- Insights into Editorials
- Insta Revision Modules for Prelims
- Current Affairs Quiz
- Static Quiz
- Current Affairs RTM
- Insta-DART(CSAT)
- Insta 75 Days Revision Tests for Prelims 2024
- Secure (Mains Answer writing)
- Secure Synopsis
- Ethics Case Studies
- Insta Ethics
- Weekly Essay Challenge
- Insta Revision Modules-Mains
- Insta 75 Days Revision Tests for Mains
- Secure (Archive)
- Anthropology
- Law Optional
- Kannada Literature
- Public Administration
- English Literature
- Medical Science
- Mathematics
- Commerce & Accountancy
- Monthly Magazine: CURRENT AFFAIRS 30
- Content for Mains Enrichment (CME)
- InstaMaps: Important Places in News
- Weekly CA Magazine
- The PRIME Magazine
- Insta Revision Modules-Prelims
- Insta-DART(CSAT) Quiz
- Insta 75 days Revision Tests for Prelims 2022
- Insights SECURE(Mains Answer Writing)
- Interview Transcripts
- Previous Years' Question Papers-Prelims
- Answer Keys for Prelims PYQs
- Solve Prelims PYQs
- Previous Years' Question Papers-Mains
- UPSC CSE Syllabus
- Toppers from Insights IAS
- Testimonials
- Felicitation
- UPSC Results
- Indian Heritage & Culture
- Ancient Indian History
- Medieval Indian History
- Modern Indian History
- World History
- World Geography
- Indian Geography
- Indian Society
- Social Justice
- International Relations
- Agriculture
- Environment & Ecology
- Disaster Management
- Science & Technology
- Security Issues
- Ethics, Integrity and Aptitude

- Indian Heritage & Culture
- Enivornment & Ecology

Insights SECURE SYNOPSIS: 9 May 2020
NOTE : Please remember that following ‘answers’ are NOT ‘model answers’. They are NOT synopsis too if we go by definition of the term. What we are providing is content that both meets demand of the question and at the same time gives you extra points in the form of background information.
2. Critically examine the economics of Alcohol addiction in the countr (250 words)
Reference: Indian Express
Introduction:
Alcohol is the most abused substance in India, according to the findings of a report “Magnitude of Substance Use in India” , submitted by AIIMS in Feb 2019 to Ministry of Social Justice and Empowerment. There are believed to be 62.5 million people in India who at least occasionally drink alcohol. Unlike many western countries the consumption of alcohol in India is witnessing a dramatic rise – for instance, between 1970 and 1995 there was a 106.7% increase in the per capita consumption. India has also become one of the largest producers of alcohol – it produces 65% of alcoholic beverages in South-East Asia. Most urban areas have witnessed an explosion in the number of bars and nightclubs that have opened in recent years.
As the lockdown eased in India, and social distancing went for a toss at alcohol outlets and there were stampedes was caused by the ineptness.
Drinking Statistics for India:
- The per capita alcohol consumption in India increased two folds between 2005 and 2016, according to the Global status report on alcohol and health 2018 released by the World Health Organization (WHO)
- Indians consumed 2.4 liters of alcohol in 2005, which increased to 4.3 liters in 2010 and scaled up to 5.7 liters in 2016, the report said.
- According to the report, the highest increase in alcohol consumption is expected in South-East Asia, with an increase of 2.2 liters in India alone, from 2005 to 2016.
- More than 3 million people died as a result of harmful use of alcohol in 2016, the report said. More than three quarters of those reported dead were men.
- Overall, the harmful use of alcohol causes more than 5% of the global disease burden.
- In the past two decades the number of people who have consumed alcohol has moved from 1 in 300 to 1 in 20.
Economics of Alcohol addiction in India:
- Alcohol is a subject in the State list under the seventh schedule of the Indian Constitution.
- Article 47 of the Directive Principle in the Constitution of India states that “The state shall undertake rules to bring about prohibition of the consumption except for medicinal purposes of intoxicating drinks and of drugs which are injurious to health.”
- Manufacture and sale of liquor is one of the major sources of their revenue, and the reopening comes at a time when the states have been struggling to fill their coffers amid the disruption on account of the lockdown.
- Like in Russia, it is difficult to wean many states away from the political economy of alcohol.
- It lubricates not just the state coffers but whole political machines.
- The Delhi government announced a 70% hike in the price of liquor across categories in the capital. Delhi’s “special corona fee” on alcohol underlines the importance of liquor to the economy of the states.
- Generally, states levy excise duty on manufacture and sale of liquor. Some states, for example Tamil Nadu, also impose VAT (value added tax).
- States also charge special fees on imported foreign liquor; transport fee; and label & brand registration charges.
- A few states, such as Uttar Pradesh, have imposed a “special duty on liquor” to collect funds for special purposes, such as maintenance of stray cattle.
- A report published by the Reserve Bank of India last September (‘State Finances: A Study of Budgets of 2019-20’) shows that state excise duty on alcohol accounts for around 10-15 per cent of Own Tax Revenue of a majority of states.
- On an average, the states collected about Rs 12,500 crore per month from excise on liquor in 2018-19, which rose to about Rs 15,000 crore per month in 2019-20, and which was further expected to cross Rs 15,000 crore per month in the current financial year.
- Alcohol has also migrated from being a question of personal freedom and choice to an issue in broader cultural wars, an odd site on which we measure progressivism in India. It is also a window on how liberalism has been misunderstood.
Challenges posed by economics of alcoholism:
- Alcohol abuse imposes large “external” costs on others.
- The deleterious effects of alcohol consumption on health and safety constitute a substantial economic burden, reducing our overall standard of living.
- The Lancet reported that more than half of those who consume alcohol in India would fall into the category of hazardous drinking.
- Chronic heavy drinking causes organ damage that results in disability and early death. Other possible consequences include cognitive impairment, addiction, reduced productivity, neglect of family responsibilities, and birth defects.
- The acute effects of alcohol abuse are still more costly: traumatic injury and property damage from accidents, criminal victimization, domestic violence, unwanted sexual encounters and venereal diseases, and hangover.
- It has been suggested that there are a worryingly 14 million people in India who would be described as dependent on alcohol and in need of help.
- Another concern is the increasing tendency to engage in binge drinking where people deliberately become intoxicated.
- Far too many people, their families and communities suffer the consequences of the harmful use of alcohol through violence, injuries, mental health problems and diseases such as cancer and stroke.
- Suffering and deprivation: People in the lower income group who cannot have an adequate amount of food, take alcohol to sleep or relax.
- More and more children are taking to alcohol consumption and the highest percentage of children who are addicted to alcohol are in Punjab followed by West Bengal and Uttar Pradesh
Way forward:
- The issue of public health is another dimension that needs to be explicitly addressed while framing a comprehensive liquor policy. This requires a two-pronged approach, one aimed at addressing alcohol-related illnesses and addictions and another aimed at putting preventive measures in place.
- The aura of shame attached to drinking and the moral condemnation of drinkers, especially by medical and social service personnel, needs to be addressed as it can be a major deterrent to seeking help.
- The medical fraternity needs to be educated in rapidly responding to and treating victims of liquor tragedies
- Addiction should not be seen as a character flaw, but as an ailment that any other person could be struggling with. Therefore, the stigma associated with drug taking needs to be reduced. Society needs to understand that alcoholics are victims and not criminals.
- Radical political decisions like that one of alcohol prohibition in Bihar may be another solution. When people do not exercise self-control, a state has to step in, as part of the Directive Principles of State Policy (Article 47).
- Education curriculum should include chapters on drug addiction, its impact and also on de-addiction. Proper Counselling is another alternative.
- Alcoholism and Drug Information Centre is devoted to prevention and treatment of substance abuse in India. They are a good resource to turn to for information and advice.
- Alcoholics Anonymous has meetings in many locations in India. This fellowship uses the 12 Steps to allow the individual to develop a better life away from addiction.
- Youth Veerangnayen focuses its efforts on educating young people about the dangers of substance abuse and helping them deal with other social problems.
- Many people are leaving India in order to seek treatment for their alcoholism abroad. The most respected alcohol and drug abuse treatment facility in Asia is DARA Rehab.
Conclusion:
Education on intelligent drinking, community intervention, regulating outlet density of alcohol shops, greater control over surrogate advertising, franker social conversation is the need of the hour to tackle alcoholism in India. Research shows that a “multiple-component approach” works best to tackle alcohol-related problems than a single-component or “stand-alone” intervention.
3. Discuss the role played by and the key objectives of integrated disease surveillance programme (IDSP) of government of India. (GS-2)
Reference: Hindustan Times
The Integrated Disease Surveillance Project was launched by the Ministry of Health and Family Welfare, in assistance with the World Bank, in 2004. It continued as the Integrated Disease Surveillance Programme (IDSP) during 12th Plan (2012–17) under the National Health Mission with a domestic budget. Under it, a Central Surveillance Unit (CSU) at Delhi, State Surveillance Units (SSU) at all State/Union Territories (UTs) headquarters and District Surveillance Units (DSU) at all Districts have been established. Recently, the Integrated Disease Surveillance Programme has been activated as a response to the Covid-19 pandemic.
The objectives of the Integrated Diseases Surveillance Project (IDSP) are:
- To strengthen/maintain decentralized laboratory based IT enabled disease surveillance system for epidemic prone diseases to monitor disease trends
- To detect and respond to outbreaks in early rising phase through trained Rapid Response Team (RRTs).
- Prevention of further transmission of disease
- Limiting mortality and morbidity
- Assessment of public health importance
- Analysis of trends of a particular disease’s outbreak
- Demonstrate the importance of public health interventions
- Allocate funds for healthcare
- Monitoring of preventive and control measures
- Identification of risk factors and developing hypothesis
- Identification of high groups and geographical areas
Components of the programme:
- Integration and decentralization of surveillance activities through establishment of surveillance units at Centre, State and District level.
- Human Resource Development – Training of State Surveillance Officers, District Surveillance Officers, Rapid Response Team and other Medical and Paramedical staff on principles of disease surveillance.
- Use of Information Communication Technology for collection, collation, compilation, analysis and dissemination of data.
- Strengthening of public health laboratories.
- Inter sectoral Co-ordination for zoonotic diseases
- Under Integrated Disease Surveillance Project (IDSP), financial and technical assistance is provided to State Governments for implementation of disease surveillance activities .
The achievements and major findings under IDSP include the following:
- IDSP has established State Surveillance Units and District Surveillance Units in all the states and District headquarters.
- Rapid Response Teams (RRT) for investigation of outbreaks and response thereto have been formed in all district and state headquarters.
- Nation-wide IT network has been established for monitoring disease surveillance activities
- 24X7 call centre (toll free no. 1075) has been established for reporting unusual health events by the community.
- Over 82% districts are electronically generating weekly surveillance reports, for early warning signals and effective timely response to disease outbreaks.
- 799 disease outbreaks have been reported during 2009.
Role played by the IDSP:
- Helps in Controlling the Disease Outbreak
- Data is collected on epidemic prone diseases on a weekly basis.
- The weekly data gives information on the disease trends and seasonality of diseases.
- The information is collected on three specified reporting formats, namely “S” (suspected cases), “P” (presumptive cases) and “L” (laboratory confirmed cases) filled by Health Workers, Clinicians and Laboratory staff respectively.
- Whenever there is a rising trend of illnesses in any area, it is investigated by the RRT to diagnose and control the outbreak.
- Identification of healthcare facilities in affected area will help to estimate their efficiency and enhance them, if needed.
- Cluster wise approach can be applied as some of the disease such as one caused by Nipah was limited to an area only.
- Real time monitoring will lead to better coordination between different levels of government and different agencies. Health, a subject mentioned in state list is always a matter of bone contention between center and state.
Real-Time monitoring of the disease and victims by the IDSP will help to cease the spread of communicable disease. Identification of area affected by a particular disease along with facilities available to combat that disease will help to contain that disease in that region.
4. Lessons learnt from the SARS epidemic have helped shape East Asian countries’ response to the Covid-19 outbr What lessons do you think can India learn from these countries? Elucidate.(250 words)
SARS infected only slightly over 8,000 people in 29 countries, with 774 deaths. Nonetheless, it shook the people and governments in East Asia out of their slumber and many of them indeed did not let this crisis go to waste. Considered a major public health crisis at the time, SARS pales in comparison to the current Covid-19 crisis in terms of both spread and impact.
Reforms undertaken during previous pandemics:
- China recognised the weakness of its health system and adopted a two-pronged approach of strengthening its government health facilities and expanding health coverage through social health insurance
- Government health expenditure tripled in a few years’ time and almost entire population received health assurance.
- Other countries, even smaller countries like Laos and Cambodia, also invested heavily in their public health systems, improved their surveillance and reporting capacities, and significantly increased their health sector budgets.
- A healthy demand for large loan projects in the health sector ensued.
- For example, Vietnam borrowed heavily to establish a strong and interlinked laboratory system covering the entire country.
- SARS, and subsequently H1N1, also prompted East Asian countries to deepen their regional cooperation on pandemic preparedness and response.
- Coordinated by the Association of South-East Asian Nations and other international development agencies, systems and agreements were put in place to identify emerging health emergencies and share information.
- SARS also provided a major push to the World Health Organization’s effort to revise the International Health Regulations (IHR) to make them more effective.
- The revisions allowed WHO to seek information from member states and mandated sharing of any epidemic information with neighbours.
Lessons learnt by East Asian countries from SARS epidemic:
- These countries, despite being closely connected with China through trade, tourism, culture and the diaspora and having ageing populations, have seen a relatively modest impact of the pandemic.
- While further research will tell us more, anecdotal evidence suggests that the widespread hygienic and face-covering practices and strong public health systems have helped in this process.
- Many of these practices and systems developed as a response to SARS, H1N1 and MERS.
- These reforms have definitely helped East Asian countries in effectively dealing with the Covid-19 pandemic.
- In East Asia, most people now press elevator buttons with a finger knuckle, avoiding direct contact with their fingertips.
- People are also more careful and use more hygienic sense in using public restrooms. Frequent handwashing is a norm.
- In places like China, Hong Kong, Taiwan, Japan and Korea, the use of face coverings in public places became the norm.
- The practice was continued even after the outbreak was over. People with coughs and colds attend office with face coverings.
- SARS also prompted some introspection about working and travel arrangements.
- Faced with temporary travel restrictions during the epidemic, the Asian Development Bank experimented with undertaking loan negotiations through videoconferencing. This turned out to be as efficient as face-to-face meetings and has now become the norm.
- A realisation set in that much of business travel could be severally rationalised.
Lessons that India can learn from these countries:
- Lives, social practices, working arrangements and the health sector will surely irreversibly change with the Covid-19 crisis in our country as well.
- The extent to which handwashing and other hygienic and physical distancing practices become part of our lifestyles
- our work arrangements change, with greater reliance on technology-enabled conferencing and supervision and reduced travel.
- access to healthcare increase through enhanced use of telemedicine.
- our disease reporting and surveillance systems must become stronger.
- Our expenditure on health comped to our peer nations should be increased.
These reforms have definitely helped East Asian countries in effectively dealing with the Covid-19 pandemic. India with its high population density must adapt the behavioural changes to curb the spread of COVID-19 pandemic. India must also undertake immediate reforms to strengthen the much needed medical infrastructure to tackle the fragile healthcare system of India.
5. The recent Vizag chemical leak incident is a wake-up call to ensure industrial safety in the countr Discuss. (250 words)
The gas leak from a chemical factory in Vizag, which killed 12 people, is the most serious of three industrial accidents that have taken place since the national lockdown was eased on May 3. The other two were in Tamil Nadu and Chhattisgarh. Though the numbers are far smaller, the tragedy brings back memories of the Bhopal gas leak, the worst industrial disaster in the world, which killed at least 3,800 people. The Vizag plant leak was styrene, a benzene derivative used to manufacture plastics and resin.
India’s industrial safety record has been patchy at the best of times. Now in the aftermath of the lockdown, it is likely to get further eroded.
Need for Industrial safety in India:
- What happened in Vizag should be considered a warning for other industries which are resuming operations after a lengthy lockdown. India’s industrial safety record has been patchy at the best of times.
- Thirty-six years after the Bhopal disaster, it is distressing to see accidents from hazardous industries.
- The fields of occupational and environmental medicine, toxicology, and epidemiology which study and prevent industrial accidents have still not been developed adequately to cater for the amount of industrial development that has occurred in India.
- Reports suggest that the Vizag plant has functioned without proper environmental clearances for a substantial period since it was set up.
- It must also be asked how the South Korean petrochemical giant, which owns LG polymers, the site of the accident, did not ensure that qualified people were in place to check systems and open the plant.
- A majority of accidents that occur in refineries are the result of human error. Often times a worker fails to follow the safety procedures that have been put into place by the company.
- The common reasons for accidents in chemical plants occur is from improper maintenance of equipment. A piece of equipment can ultimately fail and malfunction if it is not properly maintained. This can be very hazardous for the workers who are operating and working around the machine.
- Every year 48000 fatal accidents occur in India. Only 20% working population was covered under any occupational safety regulation.
- For instance, fire crackers Factory at Batle Punjab claimed 23 lives this year; Sivakashi factory explosion – 2012, 40 died and 70 injured.
Measures needed to strengthen the Industrial safety in India:
- Industries must comply with regulations, and the government must ensure that they are strictly enforced.
- Regular maintenance at scheduled intervals and the manufacturer’s recommendations is important to ensure that the equipment runs smoothly and safely.
- Employees should be properly taught on how to operate the equipment in the way it was designed to be used. They should also learn to employ safety procedures when they are operating a piece of equipment.
- Also, employees should be well versed in what to do if something goes wrong so that they can fix it before it gets out of control.
- The Occupational Safety, Health and Working Conditions Code, 2019 , which unfortunately, successive governments have not felt it necessary to ratify should be taken up and put into place immediately.
- With the ultimate aim of extending the safety and healthy working conditions to all workforce of the country, the Code enhances the ambit of provisions of safety, health, welfare and working conditions from existing about 9 major sectors to all establishments having 10 or more employees.
- It is evident that the Occupational Safety, Health and Working Conditions has some unique new initiatives for both workers and employers.
- It promotes health, safety, welfare and better working conditions of workforce by enhancing the ambit of a dynamic legislation as compared to the existing sectoral approach limited to few sectors.
- Besides, it also drastically rationalizes the compliance mechanism with one license, one registration and one return for the establishments under the ambit of the Code thereby saving resources and efforts of the employers.
- Thus, there is a need to balance the requirements of worker and employer and is beneficial to both the constituents of the world of work.
6. Briefly distinguish Hindu ethics from hedonism, utilitarianism and Kantianism. (250 words)
Reference: Ethics by Lexicon Publications
Hindu ethics are taught by guidance from leaders and teachers (guru), wandering holy men (sadhus), and sages (rishis). Sacred scriptures also give guidance. Morality is taught through Hindu scriptures, for example the Ramayana. The scriptures prohibit murder, theft, adultery, and consuming alcohol, and promote kindness to others, respect for all life (ahimsa), vegetarianism, and respect for elders. There is no centralized religious authority, and the religion is held together by the duties of family and caste
Hindu ethics is mainly subjective or personal , its purpose being to eliminate such mental impurities as greed and egoism, for the ultimate attainment of the highest good. Objective ethics, which deals with social welfare, has also been considered by Hindu thinkers. It is based upon the Hindu conception of Dharma, or duty, related to a man’s position in society and his stage in life. Objective ethics, according to the Hindu view, is a means to an end, its purpose being to help the members of society to rid themselves of self-centeredness, cruelty, greed, and other vices, and thus to create an environment helpful to the pursuit of the highest good, which transcends society. Hinduism further speaks of certain universal ethical principles which apply to all human beings irrespective of their position in society or stage in life.
It is the belief that pleasure, or the absence of pain, is the most important principle in determining the morality of a potential course of action. Pleasure can be things like “sex, drugs, and rock ’n’ roll,” but it can also include any intrinsically valuable experience like reading a good book.
Hedonism is a type of consequentialism , and it has several forms. For example, normative hedonism is the idea that pleasure should be people’s primary motivation. On the other hand, motivational hedonism says that only pleasure and pain cause people to do what they do.
Egotistical hedonism requires a person to consider only his or her own pleasure in making choices. Conversely, altruistic hedonism says that the creation of pleasure for all people is the best way to measure if an action is ethical.
Utilitarianism:
Utilitarianism as an ethical philosophy can simply be defined as a system in which ‘the theory that the rightness or wrongness of an action is determined by its usefulness in bringing about the most happiness of all those affected by it.’
Utilitarianism is allegedly the foundations of our legal system , so it is important to ask ourselves whether it is actually fair or whether some are denied the simple right to have their own interests respected.
For instance, Utilitarianism cannot be applied to entities that do not have the capacity to feel pleasure and pain or at least to have recognizable goals that they are aware of fulfilling. This debatably does not include some animals, advanced AI, the planet as a whole, a deity or the victory conditions of an overall storyline, game or narrative. Many people will argue that they should be ascribed certain rights or their interests recognized.
Kantianism:
Deontology is also referred to as duty-based ethics . It is an approach to ethics that addresses whether the motives behind certain actions are right or wrong instead of focusing on whether the results of the action are right or wrong . It is based on each individual’s duty or obligation towards each other, all living things, and the environment based on moral beliefs and values. It teaches about always acting in good faith and adheres to the Golden Rule to treat others the way you want to be treated by them .
The Ten Commandments are examples of deontology. They are moral duties that we have been taught since we were children, and we are moulded by them in the way that we should treat others, to be fair and not using them to serve selfish intentions.
7. Write short notes on; (i) Nishkama Karma (ii) ‘pride’ in Jain morality (iii) soul force (iv) Bread labour. (250 words)
Reference: Ethics, Integrity & Aptitude – G Subba Rao & P N Roy Chowdhury.
Nishkama karma:
Nishkam Karma is a central theme in the Bhagavad Gita. An important philosophical concept in Karma yoga, it means to act unselfishly, or without personal gain in mind. When acting out of Nishkam Karma, an individual is acting without any expectation that good will be returned to him/her. In Sanskrit, nishkam means “action without motive,” “work without desire” or “desire-less.”
Nishkam Karma is the opposite of Sakam Karma and is considered to be selfless action without even the subtle internal hope for a “thank you” or goodness returned. Karma Yoga focuses on the perfect alignment of thought, word and deed. A subtle ideal is embedded in this concept that encourages an individual towards an overall perfection through the path of action. Nishkam Karma is considered non-attachment to the result of personal actions in life, but with selfless and loving motives. It teaches that a spiritual seeker should act according to his dharma (duty), without being attached to the fruits or personal consequences of such work. It shows how one can live in this world and work in a manner that benefits oneself and the milieu in which he is placed. Man’s action is necessary to maintain world order and this cannot happen if one withdraws from the environment and remains idle in the name of meditation or Jnana. Desire for specific gains will cause bondage, but deeds done with a sense of dedication and in the spirit of service to God free one from such bondage.
Example: On the battlefield, Krishna told Arjuna, “Do your duty without thinking about the outcome.” What he meant was, one cannot be sure about the results and hence must not think about the outcomes, when one is performing his/her duty. One may or may not attain the desired result in the end, but thinking in a loop about the possible outcomes will only pile to the confusion, make one doubtful, distracted and increase chances of failures!
The donation or charity done to the less fortunate of the society must not be based on the fame a person receives at the end of it. Rather, the pure joy of giving, sense of satisfaction that someone’s life is more comfortable now should be the motive. It applies to CSR, NGOs, HNIs too.
‘pride’ in Jain morality:
According to the Jaina philosophy, liberation comes from the complete conquest of their internal enemies such as desire, attachment, greed, anger, and pride. This can be achieved by adhering to the three main principles of Jainism: non-violence, non-absolutism, and non-possessiveness.
Many ethical codes have condemned pride as a “deadly sin,” as part and parcel of their advocacy of moral ideals that are incompatible with life and happiness. To sustain a moral ideal that runs contrary to real human needs, these ethics have made a virtue of humility, the antithesis of pride. Pride is sinful because it presumes the moral sufficiency of man. Pride implies the sanctity of an unbroken spirit.
As an orientation toward the future, pride consists in taking responsibility for enhancing one’s self-esteem, for building one’s character, for being worthy of life. It means striving for moral and therefore existential improvement, with oneself as the beneficiary. For example, this means taking responsibility for one’s material success and professional development by seeing to it that one pursues an enriching career or series of careers, and taking responsibility for one’s spiritual enrichment by seeking out the kind of art, ideas, and relationships that it requires. A person of pride does not wait for others to fulfill his dreams for him, nor does he restrict his aspirations to what others demand. His credo is “I will do it” and “it will be good.”
soul force:
Soul force can be defined as Spiritual energy, a vital force conceived of as constituting, residing in, or emanating from the soul. Gandhi described it as follows: I have also called it love-force or soul-force.
Soulforce originally hewed to the philosophy of nonviolence as gleaned through the studies by our founding members of the legacies of several practitioners, including the Catholic Workers Movement, Cesar Chavez and the United Farm Workers Movement, Mahatma Gandhi and the struggle for Indian independence, and Dr. Martin Luther King, Jr. and the struggle for civil rights in the U.S.
Like Gandhi, King recognized the futility of confronting a dominating violent kingdom with the same weapons it had engineered and mastered. He also knew that the struggle against the illusion of ethnic supremacy was deeply rooted in the pit of hell, and victory would only be assured if the oppressed chose to fight with weapons from the heavenly arsenal.
Bread labour:
Earn thy bread by the sweat of the brow- says Bible. Bread labour means that everyone is expected to perform sufficient body-labour in order to entitle him to his living. It is not, therefore, necessary to earn one’s living by bread labour, taking living’ in its broader sense. But everyone must perform some useful body-labour.
Gandhiji said that sharirashrama , physical labour and effort, was more important for maintaining the health of the society than it was for staying physically fit. He got his ideas from Leo Tolstoy and John Ruskin and made place for bread labour in his life. Behind it was also an attempt to introduce a revolutionary idea about work.
The economics of Bread labour are the living way of life. It means that every man has to labour with his body for his food and clothing. If I can convince the people of the value and necessity of bread-labour, there never will be any want of bread and cloth.
The idea is that every healthy individual must labour enough for his food and his intellectual faculties must be exercised not in order to obtain a living or amass a fortune, but only in the service of mankind. If this principle is observed everywhere, all men would be equal, none would starve and world would be saved from a sin.

- Our Mission, Vision & Values
- Director’s Desk
- Commerce & Accountancy
- Previous Years’ Question Papers-Prelims
- Previous Years’ Question Papers-Mains
- Environment & Ecology
- Science & Technology
Drug and Alcoholism in India
- That’s all drugs and alcohol do, they cut off your emotions in the end. – Ringo Starr
- There’s not a drug on Earth that can make life meaningful.
- Drugs are a waste of time. They destroy your memory and your self-respect and everything that goes along with your self-esteem.” – Kurt Cobain
- Growing Drugs and alcohol consumption in India is becoming a major health hazard and a social menace.
- State like Punjab, North – Eastern States, Jammu & Kashmir have become home of drug abuse.
- Hooch Tragedy :
- In recent incident, over 40 people died in Gujarat’s Botad district
- 7 years since Bihar liquor ban: 199 deaths, 30 hooch cases (Police dat)
- These highlights the limitations of prohibition in addressing it; calling for a change in approach to address growing alcohol consumption
Stakeholders
Ethical Skillset for a civil servant while taking action
- Emotional Intelligence: To understand and manage the emotions of individuals and communications regarding alocohol consumption.
- Compassion: Towards women and children who face most of the social violence due to Alcoholism.
- Selflessness: To ensure action taken on public interests .
- Leadership skills: To influence people’s attitude and persuade them to overcome the bad habits of alcoholism through diligence.
Way Forwards
- Progressive Laws : These encourage responsible behavior and compliance while being strong against domestic violence, drunk driving or illegal liquor industry or its smuggling.
- Ex. Uniform drinking age law across the country where no person below that should be permitted to buy alcohol.
- Regulations over liquor Industry: It will avoid indirect marketing tactics to promote liquor consumption (e.g., surrogate marketing) and also curb illicit liquor production.
- This could avert hootch tragedy which frequently occurs in states like Bihar, Gujarat etc.
- Labeling Standards: With adequate notices and cautions to help people in making informed decisions.
- Avoiding Arbitrary or Discretionary actions : while containing negative fallouts of prohibition on tourism and MICE (meetings, incentives, conferences and exhibitions) sector.
- Use of Corporate Social Responsibility: To ensure responsible drinking and increasing the de-addiction facilities.
- Community Participation: Gathering community support to avoid addiction and rehabilitate people suffering from addiction.
- Awareness : Information, Education and Awareness (IEC) campaigns from state and district administration to educate people about the ill effects of alcoholism.
Answer our survey to get FREE CONTENT
Feel free to get in touch! We will get back to you shortly
- Privacy Policy
- Terms of Service
- Quality Enrichment Program (QEP)
- Total Enrichment Program (TEP)
- Ethics Marks Maximization Program
- Interview Mentorship Program (IMP)
- Prelims Crash Course for UPSC 2024
- Science of Answer Writing (SAW)
- Intensive News Analysis (INA)
- Topper's UPSC PYQ Answer
- Essay Marks Maximization Program
- PSIR Optional
- NEEV GS + CSAT Foundation
- News-CRUX-10
- Daily Headlines
- Geo. Optional Monthly Editorials
- Past Papers
- © Copyright 2024 - theIAShub
Talk To Our Counsellor
- International
- Today’s Paper
- Premium Stories
- Express Shorts
- Lok Sabha polls Live
- JAC 10th Result
- Board Exam Results
UPSC Essentials: Case Study of the week- Fight for a drug-free community
Every youth who destroys his life by drug addiction is a loss to our society. the solution-oriented case study discusses the issue of drug abuse and de-addiction programme that aspirants will find useful in gs i, essay and ethics. solve the mcq given below after reading this article..
An article that fits as a case study is a story from The Indian Express . “In Arunachal district, women lead the fight for the drug-free community” written by Tora Agarwala. A solution-oriented story discusses a successful campaign against drug abuse in Changlang, Arunachal Pradesh. Led by women, the initiative titled “Nasha Mukt Changlang”, also shows how the dedicated district administration achieved its goal with the support of other stakeholders.

Case studies are an important part of the UPSC civil services exam, especially the ethics paper. These case studies can also be very beneficial for value addition in the essay, GS mains and interview. This particular case study is relevant for GS I- Issues related to women, youth, drug addiction. Also, recently United Nations Office on Drugs and Crime (UNODC) released its World Drug Report 2022 on World Drug Day. Use the case study wisely and enrich your answers. (Solve the MCQ given at the end of the article.)
“Every youth who destroy his life by drug addiction is a loss for our society”. For 25 long years, Kimcham Taiju’s husband in the Changlang district of Arunachal Pradesh was addicted to ‘kaani’ which is opium in Arunachal Pradesh. Located in India’s eastern most periphery, Changlang of Arunachal Pradesh has long contended with an addiction problem. In 2021, a survey on substance abuse conducted by the Ministry of Social Justice and Empowerment identified the Changlang district of Arunachal Pradesh as among the 272 most vulnerable in the country. This has led the district administration to try to find a solution to this big problem.
Drug addiction problem and the fight against it. To fight against this serious issue there is a need for administration, civil societies and individuals to come together- not just for treatment but also rehabilitation.
The problem
1. Addiction is a problem that has its roots in colonial times. “The British encouraged the Singphos (in the northern region of the district) to consume opium to subjugate them. In Tangsa (tribe) areas, near Myanmar, black salt was traded for opium. This led to addiction in the local population. Soon, other synthetic drugs made inroads”- Deputy Commissioner of Changlang.

2. Several government-sponsored de-addiction camps were carried out without much success in the past. Most of them were traditional in nature with less participation from other stakeholders, other than the government.
3. Changlang and the two neighboring districts of Tirap and Longding (colloquially referred to as part of the TLC belt) have long been caught in a cycle of drugs and insurgencies: militant groups trade opium for arms. Despite multiple crackdowns by government agencies over the years, opium continues to thrive, with plantations across these areas.
The stakeholders
Drug addicts, district administration, women SHGs, gram sabha, NGOs, livelihood providers (for those who return after treatment), every individual etc.
The solutions
1. Bottom-up approach: A change in approach from the traditional unsuccessful past. Differently formulated de-addiction programme which would be bottom-up, and in collaboration with the village. In a bottom-up approach, there is a willingness to solve problems by creating fluidly. There is no imposition of structure. Every individual is seen as a stakeholder and participates in the mission.
2. Role of SHGs and Gram Sabha: Deputy Commissioner directed the women to activate their Self Help Group (SHG) network, and hold a gram sabha meeting, presided by village elders, where the issue was discussed, a list of addicts drawn up, and the idea of de-addiction suggested. At the end of the meeting, a unanimous resolution was passed: an undertaking by the village to be “drug-free”.
3. “Nasha Mukt Changlang” initiative- Like ” Nasha Mukt Bharat” on a micro-scale, it targeted the entire village, instead of a single individual. The addicts would be sent for a month-long de-addiction programme, either at a pre-existing NGO-run health facility or a temporary one in the village, followed by post-treatment rehabilitation including government-sponsored livelihood opportunities as well as counseling sessions and Narcotics Anonymous meetings.
As alternative livelihood options for those who have returned from the camps, the administration has provided recovering villages with poultry, piggery, and mushroom units to keep them busy.
So, “Nasha Mukta Chalang comprised” of (can be used in your answers and case studies solutions)
—Month long de-addiction programme at a de-addiction facility.
—Post-treatment rehabilitation and government-sponsored livelihood opportunities
—Counseling sessions
—Narcotics Anonymous meetings.
4. Close synergy between local communities and authorities- Success is possible due to the close synergy between the local community and the authorities. As the administration is involved things were seen to be more “systematic”.
5. Initiative by individuals -The story mentions Kitnya. Kitnya is the administration’s point of contact on the ground for villages under two circles, Yatdam and Namtok. From persuading people to join the camps, to coordinating with local SHGs, to supervising the day-to-day running of the centers, Kitnya spends hours in voluntary service.
6. Treat the problem as social, not criminal- “We did not treat the issue as a law and order problem. With addicts, treat them as patients and not as criminals because addiction is a medical problem. They need patience and care.” Positive sign- reports of some who relapsed, post-treatment.
7. Pro-active role of administration- It is seen by the efforts of administration right from the time when a group of women approached the district’s then Deputy Commissioner, Devansh Yadav, in February 2021, seeking a solution. The administration and the deputy commissioner realised that out-of-box thinking is required. It was realised that the administration has to walk hand in hand with the SHGs, Women groups, gram sabha and the village as a whole. The Deputy Commissioner says, “Since everyone in the village is involved, it is easy to identify them and work with them again.”
Interesting narration ( fit for an essay anecdote)
Kimcham Taiju says, she made the “bravest decision” of her life: she signed up her husband for a drug de-addiction programme. One Sunday evening in March, Taiju and the other women of the village gathered at the local community hall, and decided that “enough was enough”. A list of 50 names was drawn up, and submitted for the district administration’s month-long drug de-addiction programme. That night, Taiju broke the news to her husband. “Jaabi ne? (Will you go),” Taiju recalls asking him. “Jaam de (I will),” was his answer. The men were sent 100 km away, to a de-addiction facility in Bordumsa town. The women say the plan worked because “no one was singled out”. “They knew they were going together,” says Taijong, in her 40s.
Beyond the case –
1. The International Day against Drug Abuse and Illicit Trafficking, or World Drug Day , is marked on 26 June every year to strengthen action and cooperation in achieving a world free of drug abuse.
2. This year the theme is “Addressing drug challenges in health and humanitarian crises”. The focus of the United Nations Office On Drug And Crime (UNODC) is to spread awareness about it so that a world free of drug abuse can be created. The motive is to fight off misinformation by sharing facts and by providing methods of treatment, prevention and care.
3. Recently, United Nations Office on Drugs and Crime (UNODC) released its World Drug Report 2022 on World Drug Day. In 2021, drugs accounted for 91 percent of all sales on the 28 major darknet marketplaces, up from 85 percent in 2019.
Initiatives of the Government of India against drug abuse
1. National Action Plan for Drug Demand Reduction (NAPDDR) for 2018-2025. It aims to reduce the adverse consequences of drug abuse through a multi-pronged strategy involving education, de-addiction and rehabilitation of affected individuals and their families.
2. Narcotic Drugs and Psychotropic Substances (NDPS) Act To prevent and combat drug abuse and illicit trafficking, with an apparent emphasis on supply reduction.
3. The National Fund for Control of Drug Abuse.
4. The Mental Health Care Act (2017) has included alcohol and drug use disorders under its ambit.
5. NCPCR-NCB released an action plan to combat drug abuse among children
The plan has been conceptualised as a framework to wean children away from drug abuse and stop the sale of drugs near schools and educational and childcare institutions.
Point to ponder
If you were a civil servant what will you do to tackle drug addiction among youth in your area on the social front?
Which of the following statement is true:
1. Theme for International Day against Drug Abuse and Illicit Trafficking 2022 is Addressing drug challenges in health and humanitarian crises.
2. The Mental Health Care Act (2017) includes alcohol and drug use disorders under its ambit.
3. India is a signatory to Illicit Traffic in Narcotic Drugs and Psychotropic Substances, 1988.
4. According to the World Drug Report 2022, there has been an acceleration in the use of cannabis in some areas of the world.
a) 1 and 2 b) 1, 2 and 3 c) 2 and 4 d) All are correct
Answer for the previous MCQ-
UPSC Essentials: One word a day— Dumping- (c)

Can UP interfaith live-in couples get police protection? Subscriber Only

Heart disease & maternal deaths: New ICMR study attempts to Subscriber Only

When EC overcame 'impossible' challenge, held second LS polls timely Subscriber Only

UPSC Key | FDI in space sector, heavy rainfall in Subscriber Only

S Y Quraishi on life after poll bonds: The next Subscriber Only

The strategic importance of Andaman & Nicobar Islands Subscriber Only

AAP Bharuch candidate's frontline fighters are his two wives Subscriber Only

Is there hope for India’s dying wastelands? Subscriber Only

In Delhi refugee camp, a Nehru from Pak awaits citizenship Subscriber Only
- Arunachal Pradesh
- UPSC Civil Services Exam
- UPSC Essentials
- UPSC Specials

Jharkhand Academic Council (JAC) will declare the Class 10 results today (April 19) on their official websites. Students can access their scorecards by entering their login details on jac.nic.in, jharresults.nic.in, or jac.jharkhand.gov.in. The marksheet will include personal details, subject-wise marks, and a cumulative score. Last year, the pass percentage was 95.38%.
- LSG vs CSK Live Score, IPL 2024: KL Rahul's Lucknow Super Giants take on Ruturaj Gaikwad's Chennai Super Kings 15 mins ago
- Jharkhand Board JAC 10th Result 2024 Live Updates: Check at jacresults.com; East Singhbhum top performing district 37 mins ago
- Lok Sabha Election 2024 Voting Live: Blast in Chhattisgarh's Bastar kills CRPF jawan; 49.78% voter turnout till 3 pm 40 mins ago
- Delhi News Live Updates: Court reserves order on Delhi CM’s plea for medical check-ups, seeks reply from ED, Tihar jail 2 hours ago

Best of Express

Buzzing Now

Apr 19: Latest News
- 01 Sule has borrowed money from Sunetra Pawar, does not own a vehicle, shows election affidavit
- 02 IPL 2024 Points Table update: Mumbai Indians rise to 7th while Punjab Kings plummet to 9th after PBKS vs MI
- 03 Firing outside Salman’s residence: FB account used by Anmol Bishnoi to claim responsibility created the same day
- 04 At UN, Iran warns Israel against further military action
- 05 IPL 2024 Purple Cap: Jasprit Bumrah tops charts, Gerald Coetzee rises to 3rd after PBKS vs MI
- Elections 2024
- Political Pulse
- Entertainment
- Movie Review
- Newsletters
- Gold Rate Today
- Silver Rate Today
- Petrol Rate Today
- Diesel Rate Today
- Web Stories
- TRP for UPSC Personality Test
- Interview Mentorship Programme – 2023
- Daily News & Analysis
- Daily Current Affairs Quiz
- Baba’s Explainer
- Dedicated TLP Portal
- 60 Day – Rapid Revision (RaRe) Series – 2024
- English Magazines
- Hindi Magazines
- Yojana & Kurukshetra Gist
- PT20 – Prelims Test Series
- Gurukul Foundation
- Gurukul Advanced – Launching Soon
- Prelims Exclusive Programme (PEP)
- Prelims Test Series (AIPTS)
- S-ILP – English
- S-ILP – हिंदी
- Connect to Conquer(C2C) 2024
- TLP Plus – 2024
- TLP Connect – 2024
- Public Administration FC – 2024
- Anthropology Foundation Course
- Anthropology Optional Test Series
- Sociology Foundation Course – 2024
- Sociology Test Series – 2023
- Geography Optional Foundation Course
- Geography Optional Test Series – Coming Soon!
- PSIR Foundation Course
- PSIR Test Series – Coming Soon
- ‘Mission ಸಂಕಲ್ಪ’ – Prelims Crash Course
- CTI (COMMERCIAL TAX INSPECTOR) Test Series & Video Classes
- Monthly Magazine
RSTV IAS UPSC – Fighting Drug Menace
- July 4, 2019
The Big Picture- RSTV
Fighting Drug Menace
TOPIC: General Studies 2 Government policies and interventions for development in various sectors and issues arising out of their design and implementation. Structure, organization and functioning of the Executive
In News: 26 th June is celebrated as International Day against Drug Abuse and Illicit Trafficking
- The decision to mark the day was taken on 7 December 1987 through a resolution of the United Nations General Assembly in order to strengthen global action and cooperation to achieve its aim of making the international society free of drug abuse.
- This year’s theme ‘Health for Justice, Justice for Health’ emphasises that justice and health are “two sides of the same coin” when it comes to addressing the problems associated with drugs.
Drug abuse has become a universal and growing issue of concern to humanity. The illicit drugs have multiple consequences to health, society and economy. The issue is complex and multifaceted requiring both health measures and efforts to control trafficking/smuggling and manufacture of illicit drugs. A reduction in the demand of drugs of addiction both legal and illegal, which lead to numerous health, family and societal consequences, is required.
Drug Menace in India
Located between two largest opium producing regions of the world i.e. Golden Crescent in the west and Golden Triangle in the east, India is considered to be extremely vulnerable to narcotic drug trafficking.
In February 2019, AIIMS submitted its report ‘Magnitude of Substance Use in India’ that was sponsored by the Ministry of Social Justice and Empowerment. The study found that –
- Around 5 crore Indians reported to have used cannabis and opiods at the time of the survey.
- About 60 lakh people are estimated to need help for their opioid use problems
- Nationally, it is estimated that there are about 8.5 lakh people who inject drugs.
- Of the total cases estimated by the report, more than half of them are contributed by states like Assam, Delhi, Haryana, Manipur, Mizoram, Sikkim and Uttar Pradesh. Punjab ranks consistently at the top or in the top five in many of the surveys conducted.
India is a signatory of the following conventions:
- Single Convention of Narcotic Drugs 1961 as amended by the 1972 protocol
- Convention on Psychotropic Substances 1971
- UN Convention against Illicit Trafficking in Narcotic Drugs and Psychotropic Substances, 1988
India is a party to all three UN Conventions and also has ratified all of them. In India, the Narcotic Drugs and Psychotropic Substances Act (NDPS), 1985 provides the current framework for drug abuse control in country.
Steps taken by Government
- Constituted Narco-Coordination Centre (NCORD) in November, 2016 and revived the scheme of “Financial Assistance to States for Narcotics Control”.
- Narcotics Control Bureau has been provided funds for developing a new software i.e. Seizure Information Management System (SIMS) which will create a complete online database of drug offences and offenders.
- Constituted a fund called ‘National Fund for Control of Drug Abuse’ to meet the expenditure incurred in connection with combating illicit traffic in Narcotic Drugs; rehabilitating addicts, and educating public against drug abuse, etc.
- Conducting National Drug Abuse Survey to measure trends of drug abuse in India through Ministry of Social Justice & Empowerment with the help of National Drug Dependence Treatment Centre, AIIMS
- Ministry of Social Justice and Empowerment has introduced Scheme of Assistance for Prevention of Alcoholism and Substance (Drugs) Abuse . The scheme seeks to benefit victims of alcohol and substance abuse. Under the scheme, non-governmental organisations have been entrusted with the responsibility for delivery of services and the Ministry bears substantial financial responsibility (90% of the prescribed grant amount).
- The Act provides stringent provisions for the control and regulation of operations relating to narcotic drugs and psychotropic substances.
- It also provides for forfeiture of property derived from, or used in, illicit traffic in narcotic drugs and psychotropic substances.
- It also provides for death penalty in some cases where a person is a repeat offender.
Do we require a National Policy to deal with it?
India has a fairly large reservoir of raw opium, cannabis, alcohol and now synthetic opioid users, both in urban and rural areas, with a large number of them being young and adolescent population. The social, health and economic consequences of substance dependence are well known and include
Health: mortality, morbidity, psychiatric and physical disorders
Social: accidents, absenteeism, family disintegration, prostitution, organized crime etc.
Economic: finances spent on developing services, drain on national resources, loss of productivity, etc.
Way forward
- NCB in collaboration with state agencies and concerned ministries, organizes awareness campaigns. Awareness campaign is also a continuous process. Other agencies such as social welfare or health department have to also contribute in this fight against drug menace.
- De-addiction and demand reduction is important. Demand reduction is also a job that the government agencies will have to ensure. For demand reduction, there are addition centres. The ministry of social justice and empowerment gives money to some NGOs to work in this field.
- There should be rehabilitation within the society . It is difficult to get the addicted people back to creative level so government has to make necessary and sufficient rehabilitation centres with required resources to bring people back to mainstream society.
- If a common man has information about drug supply chain or peddlers or wants to inform about someone suffering from this menace, they can contact NCB. For supply reduction, they can contact state director.
- Public campaign- anti-drug consumption campaign could be launched with more vigour, starting from school children particularly of higher grades. There are marathons, walkathons on this issue. There are advertisement placed in railways and metros.
- Collaborate at international and multilateral forums so as to ensure that those foreign jurisdictions also act to stop the supply into India. There are various bilateral agreements and treaties with countries in which sharing of information and facilitating investment is also important.
- As a society, we need to say no to drugs . Make efforts to take action against them who are involved in supplying drug to drug traffickers. At least the youngsters do not fall prey to this menace in the times to come should be the aim. It is not a cool thing to do which can be done once for trial and get out of it quickly. Also, they should be made aware to not get into peer pressure.
Reforming De-addiction centres
- Budget, training of administrators and the care and empathy of the best de-addiction centres: Need to study the best practices, and replicate it by providing the appropriate training and facilities here. Minimum standard of care should be provided.
- Right of people should still be the same and not any less than that of people outside that centres. Gross violation of human rights need to be tacked on an immediate basis.
- Unregulated de-addiction centres which are not equipped to handle this problem should be banned immediately. Strict regulations should be established and zero tolerance towards misdemeanours need to be practiced .
Connecting the dots:
- Drug menace has the capacity to ruin India’s demographic dividend. Explain how India as a society and sovereign country tackle this issue.
- Examine the steps that are being taken by the Government for a better framework for the provision of de-addiction facilities? What are the various ways, according to you, in which this alarming situation can be handled?
- What are the reasons for growing drug abuse in India? Also mention the challenges and steps taken to curb this menace
For a dedicated peer group, Motivation & Quick updates, Join our official telegram channel – https://t.me/IASbabaOfficialAccount
Subscribe to our YouTube Channel HERE to watch Explainer Videos, Strategy Sessions, Toppers Talks & many more…

- IAS UPSC IASbaba RSTV Debate , RSTV Big Picture UPSC IAS
Related Posts :
Daily current affairs ias | upsc prelims and mains exam – 4th july 2019, iasbaba’s tlp – 2019 phase 2 : upsc mains general studies questions[5th july,2019] – day 15.
- DAILY CURRENT AFFAIRS IAS | UPSC Prelims and Mains Exam – 19th April 2024
- UPSC Quiz – 2024 : IASbaba’s Daily Current Affairs Quiz 19th April 2024
- [DAY 41] 60 DAY RAPID REVISION (RaRe) SERIES for UPSC Prelims 2024 – SCIENCE AND TECHNOLOGY, CURRENT AFFAIRS & CSAT TEST SERIES!
- UPSC Quiz – 2024 : IASbaba’s Daily Current Affairs Quiz 18th April 2024
- DAILY CURRENT AFFAIRS IAS | UPSC Prelims and Mains Exam – 18th April 2024
- [DAY 40] 60 DAY RAPID REVISION (RaRe) SERIES for UPSC Prelims 2024 – HISTORY, CURRENT AFFAIRS & CSAT TEST SERIES!
- DAILY CURRENT AFFAIRS IAS | UPSC Prelims and Mains Exam – 13th April 2024
- UPSC Quiz – 2024 : IASbaba’s Daily Current Affairs Quiz 17th April 2024
- [DAY 39] 60 DAY RAPID REVISION (RaRe) SERIES for UPSC Prelims 2024 – HISTORY, CURRENT AFFAIRS & CSAT TEST SERIES!
- IASbaba’s Secures Top Rank in UPSC CSE 2023 Results – Rank 1 Aditya Srivastava (IASbaba’s Flagship Program ‘ILP’ Student)
Don’t lose out on any important Post and Update. Learn everyday with Experts!!
Email Address
Search now.....
Sign up to receive regular updates.
Sign Up Now !
Digitally learn
Knowledge is Empower

About alcohol prohibition in India & its Socio-Economic effects | UPSC

Table of Contents
Alcohol prohibition and directive principles of state policy (DPSP) | UPSC -IAS
- The directive principles of state policy (DPSP) in the constitution of India (article 47) state that “the State shall endeavor to bring about prohibition of the consumption except for medicinal purposes of intoxicating drinks and of drugs which are injurious to health”.
- The Directive Principles are not-justiciable rights of the people but fundamental in the governance of the country. It shall be the duty of the State to apply these principles in making policy laws per Article 47.
- As Per Article 38, state and union governments, as duty, shall make further detailed policies and laws for implementation considering DPSPs as fundamental policy. In contrary to Article 37, many policies have been implemented by states and union government which go against the DPSPs such as using intoxicating drinks as source of major tax revenue instead of implementing prohibition for better health of people.
- When the union government feels that alcohol prohibition is no longer useful to the nation, it shall be deleted from DPSPs by bringing a constitutional amendment to remove ambiguity in policy making / direction.
- Judiciary can repeal any policy/law devised by the government which is diametrically opposite to any DPSP. An existing policy in line with DPSP can not be reversed , however it can be expanded further in line with DPSP. The policy changes applicable under DPSP shall not be reversible unless the applicable DPSP is deleted by constitutional amendment.
- Many states imposed prohibition of alcohol and later prohibition lifted to collect more revenue/taxes by the states. Lifting / relaxing prohibition of alcohol is unconstitutional which is reversing the earlier implemented policy as per Article 37 as long as alcohol prohibition is part of DPSP.
National Prohibition was advocated by Mahatma Gandhi , as well as by many Indian women. Prohibition, in the states of India that have implemented the policy, has led to lower rates of drinking among men, as well as a decreased incidence of violence against women.
Temperance movement in India | UPSC – IAS
- The temperance movement in India aims at curbing the use of alcohol in that country. In some places, the temperance movement has led to alcohol prohibition in India, with many temperance organisations continuing their work today.
- The temperance movement in India often led to the prohibition of alcohol in various states, as with Manipur. In British India, many Indian temperance activists agitated for prohibition in the country.
- Mahatma Gandhi was a champion of the temperance movement and viewed foreign rule as an obstacle to national prohibition. When India gained independence in 1947, prohibition was included in the Directive Principles of the Constitution of India and the government of several states such as Gujarat introduced it.
What are Dry days ? | UPSC – IAS
Dry Days are specific days when the sale of alcohol is prohibited. Dry Days are fixed by the respective state government. Most Indian states observe dry days on major religious festivals/occasions depending on the popularity of the festival in that region.
- National holidays such as Republic Day (26 January),
- Independence Day (15 August) and
- Gandhi Jayanti (2 October) are usually dry days throughout India.
- National dry days also occur during Election Commission of India-ordained voting and result days.
Dry days also depend on the establishment selling alcohol. For example , generally 5-star hotels do not have to observe all the dry days that liquor stores and small bars may have to. Dry days are also observed on and around voting days.
States practicing prohibition | UPSC – IAS
Alcohol prohibition in India is in force in the states of Bihar, Gujarat, Mizoram, Nagaland as well as in the union territory of Lakshadweep . All other Indian states and union territories permit the sale of alcohol.
Alcohol prohibition in Bihar | UPSC – IAS
- Bihar Chief Minister Nitish Kumar officially declared the total ban on 5 April 2016, and said in a press conference, “All type of liquor will be banned in the state from today. Sale [and consumption] of any type of alcohol in hotels, bars, clubs and any other place will be illegal from today onwards.”
Violation of law
- Violating the law carries a penalty of 5 years to 10 years imprisonment. On 30 September 2016 Patna High Court ruled that the ban is “illegal, impractical and unconstitutional”.
- Although even before the High Court order came, the Bihar government had announced that it would enforce a new stringent law from 2 October 2016, only to stay adamant on it after the order. The government had drafted a new law to keep from withdrawing the ban.
- As per the new liquor law, those found indulging in unlawful import, export, transport, manufacture, possession, sale, intoxicant or liquor could attract a minimum 10 years of jail term which may extend to imprisonment for life besides a minimum fine of Rs 1 lakh which may extend to Rs 10 lakh.
Historic Human Chain
- On 21 January 2017, more than 3 crore people of Bihar joined hands to form a historic human chain along 12,760 km of roads to support ban on alcohol by Bihar C.M Nitish Kumar. This unprecedented and massive human chain was supported by people from all walks of life and political parties.
Social and Economic effects of alcohol Prohibition in Bihar | UPSC – IAS
Prohibition, in the states of India that have implemented the policy, has led to lower rates of drinking among men, as well as a decreased incidence of violence against women. In the state of Bihar it is observed that:-
- Within a year of prohibition, the number of murders and gang robberies decreased by 20%.
- The number of riots fell by 13% and traffic accidents were reduced by 10% .
- For the economy – spending per household rose: increase in sales of milk by 10%, cheese by 200%, two-wheeled vehicles by 30%, and electrical appliances by 50%.
- In villages, brick houses are gradually taking the place of more rudimentary cottages since state Prohibition came into effect.
- At the same time, substance abuse has increased significantly due to liquor being hard to access.
Alcohol prohibition in Gujarat | UPSC – IAS
- Bombay State had prohibition between 1948 and 1950, and again from 1958. Gujarat has a sumptuary law (laws that try to regulate consumption.) in force that proscribes the manufacture, storage, sale and consumption of alcoholic beverages.
- The legislation has been in force since 1 May 1960 when Bombay State was bifurcated into the states of Maharashtra and Gujarat.
- Bombay Prohibition Act, 1949 is still in force in Gujarat state, however there is licensing regime in Maharashtra with granting licenses to vendors and traders.
- Gujarat is the only Indian state with a death penalty for the manufacture and sale of homemade liquor that results in fatalities. The legislation is titled the Bombay Prohibition (Gujarat Amendment) Act, 2009. The legislation was prompted by numerous deaths resulting from the consumption of methyl alcohol.
- Predictably, smuggling and illicit sale of alcohol are very common. “Folder” is a slang term of unknown origin, used in Gujarat to refer to a bootlegger who delivers alcohol on-demand.
Online Permits
- Foreigners and visitors from other parts of India can apply online for a permit. There are 35 stores across the state including nine in Ahmedabad that sell liquor on production of a physical copy of the permit. Once the permit expires, users are to hand-over the unconsumed liquor to the district collector.
Public Interest Litigation
- Five petitions, including Public Interest Litigation (PIL), have been filed before the Gujarat High Court challenging the prohibition law in the state. Most petitioners have raised concern that prohibition law violates Right to Privacy and are seeking relaxation on consumption in privacy.
Alcohol prohibition in Mizoram | UPSC – IAS
- The Mizoram Liquor Total Prohibition Act, 1995 banned sale and consumption of alcohol effective from 20 February 1997. In 2007, the MLTP Act was amended to allow wine to be made from guavas and grapes, but with restrictions on the alcohol content and the volume possessed. It is illegal to transport these products out of the state.
- Mizoram repealed prohibition on 10 July 2014, a period of 17 years after it had been imposed. On that date, the state Legislative Assembly passed the Mizoram Liquor (Prohibition and Control) Act, 2014 (MLPC Act), replacing the MLTP Act. The Presbyterian Church had organised mass prayers in all member churches across the state twice that year opposing the repeal of prohibition.
- The Mizoram Liquor (Prohibition and Control) Act, 2014 was repealed on 20 March 2019 with the Mizoram Liquor Prohibition Act, 2019, it was a legislation promised by the Mizo National Front. Rules are yet to be notified for the ban in the state.
Alcohol prohibition in Nagaland | UPSC- IAS
The Nagaland Liquor Total Prohibition Act, 1989 (NLTP Act) banned the sale and consumption of alcohol in 1989. Enforcement of the ban is lax and Indian Made Foreign Liquor is readily available. Authorities generally turn a blind eye towards illegal sales. Reports have stated that some police officials themselves engage in bootlegging. The Congress party has termed prohibition a “total failure” and has pleaded for it to be revoked.
- The excise department had earned around ₹600 lakh (equivalent to ₹47 crore or US$6.6 million in 2019) prior to prohibition.
- It earned about ₹10 lakh (US$14,000) annually in NLTP Act related fines as of June 2014. The Morung Express estimated that were about 500 illegal liquor bars in Dimapur, the largest city in the state, as of August 2014. Alcohol is also smuggled in from neighbouring Assam.
Alcohol prohibition in Lakshadweep | UPSC – IAS
Lakshadweep is the only union territory that bans the sale and consumption of alcohol. Consumption is permitted only on the island of Bangaram. Bangaram is an uninhabited island, but the Bangaram Island Resort has a bar.
States no longer practicing prohibition | UPSC – IAS
There are five States that no longer practicing prohibition. These states have previously enforced, but later repealed prohibition.
- Andhra Pradesh
Alcohol prohibition in Andhra Pradesh
- The total prohibition was introduced in Madras State (which included Coastal Andhra and Rayalaseema) when C. Rajagopalachari became Chief Minister in 1952. The ban was re-introduced by N. T. Rama Rao in 1994. N. Chandrababu Naidu repealed the prohibition in 1997, claiming that it was “not successful or feasible because of the leakages within the state and from across the borders”.
Alcohol prohibition in Haryana
- Bansi Lal led Haryana Vikas Party lift the prohibition on 1 April 1998. The total prohibition was in force in the state from July 1996.
Alcohol prohibition in Kerala
- Kerala currently allows alcohol to be served in most hotels, bars and airports. A ban imposed by the United Democratic Front government in 2014 was reversed by the Left Democratic Front government in 2017 when they came to power citing heavy losses in state revenue and sharp decrease in tourism industry.
- On 24 August 2014, Chief Minister Oommen Chandy announced that Kerala would implement prohibition in a phased manner. The decision was a result of factional conflict within the UDF, led by KPCC President V. M. Sudheeran. The decision was supported by the Catholic Church, Indian Union Muslim League (IUML) and the Kerala Congress. Liquor bars in Kerala are required to renew their licenses every year. The state government did not license any bars on 31 March 2014, resulting in the closure of 418 bars.
- The state government also declared its intention not to renew the licenses of the remaining 313 bars in the state. The state owned Kerala State Beverages Corporation (Bevco) had 338 shops, and Bevco would shut down 10% of them every year. Consumerfed, which has 46 shops, would also be closed. However, sale of alcohol would continue to be permitted in 5-star hotels, and there were fourteen 5-star hotels in the state as of August 2014. Toddy would also continue to be legally sold, and toddy shops would be permitted to operate as before. The state incurred heavy losses due to its tourism-based economy being severely affected by prohibition.
- However, after the 2016 Elections where the UDF was defeated by the LDF, the newly elected Chief Minister, Pinarayi Vijayan, reversed the policy of prohibition. The Chief Minister stated that the state’s policy would move from prohibition to regulation. In June 2017 the ban was revoked, allowing three stars hotels and above to openly serve alcohol to its customers.The restrictions on bars were also eased with bars being allowed to remain open till 2300 instead of previous 2200 with new bars being allowed to apply for license. Airport lounges were also allowed to start serving alcohol again.
Alcohol prohibition in Manipur
- Prohibition is enforced in the Imphal East, Imphal West, Thoubal and Bishnupur districts of Manipur. Prohibition was enforced statewide by the Raj Kumar Ranbir Singh government with effect from 1 April 1991. Local brews called ashaba and atingba are available in most areas, and authorities usually ignore their sale and consumption.
- In 2002, the Okram Ibobi Singh government lifted prohibition in the five hill districts of Manipur. The state Legislative Assemble passed the Manipur Liquor Prohibition (Amendment) Act, 2002 on 31 July 2002 lifting prohibition in the districts of Chandel, Churachandpur, Senapati, Tamenglong and Ukhrul. In 2015, Chief Minister Okram Ibobi Singh stated in the Manipur state assembly that the state government was looking at the option of lifting prohibition in the state, but liquor ban still continues in the state.
Alcohol prohibition in Tamil Nadu
- The total prohibition was introduced in Madras State when C. Rajagopalachari became Chief Minister in 1952. In 1971, the DMK government led by M. Karunanidhi suspended it on 30 August 1971 and allowed the sale of arrack and toddy.
- In 1983, after previous serial introduction of prohibition and its revocation the state owned liquor distribution company TASMAC was established by the then Chief Minister M. G. Ramachandran. The TASMAC has a monopoly over wholesale and retail vending of alcoholic beverages. Since then, various prohibitions were installed in form of reduction of TASMAC shops, however, the alcohol selling is still legal.
You may also like:

Leave a Comment Cancel reply
Notify me of follow-up comments by email.
Notify me of new posts by email.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Glob Ment Health (Camb)
Alcohol use among adolescents in India: a systematic review
Abhijit nadkarni.
1 Centre for Global Mental Health, London School of Hygiene and Tropical Medicine, Keppel Street, London, UK
2 Addictions Research Group, Sangath, Porvorim, Goa, India
3 Department of Psychology, Harvard University, 33 Kirkland Street, Cambridge, USA
Devika Gupta
Sonal gupta, urvita bhatia.
4 Oxford Brookes University, Oxford, UK
Niharika Tiwari
5 Tees, Esk and Wear Valleys NHS Foundation Trust, Darlington, UK
6 Social Finance, Tintagel House, 92 Albert Embankment, London, UK
Godwin Fernandes
Richard velleman.
7 Department of Psychology, University of Bath, Bath, UK
Associated Data
For supplementary material accompanying this paper visit https://doi.org/10.1017/gmh.2021.48.
Alcohol use is typically established during adolescence and initiation of use at a young age poses risks for short- and long-term health and social outcomes. However, there is limited understanding of the onset, progression and impact of alcohol use among adolescents in India. The aim of this review is to synthesise the evidence about prevalence, patterns and correlates of alcohol use and alcohol use disorders in adolescents from India.
Systematic review was conducted using relevant online databases, grey literature and unpublished data/outcomes from subject experts. Inclusion and exclusion criteria were developed and applied to screening rounds. Titles and abstracts were screened by two independent reviewers for eligibility, and then full texts were assessed for inclusion. Narrative synthesis of the eligible studies was conducted.
Fifty-five peer-reviewed papers and one report were eligible for inclusion in this review. Prevalence of ever or lifetime alcohol consumption ranged from 3.9% to 69.8%; and prevalence of alcohol consumption at least once in the past year ranged from 10.6% to 32.9%. The mean age for initiation of drinking ranged from 14.4 to 18.3 years. Some correlates associated with alcohol consumption included being male, older age, academic difficulties, parental use of alcohol or tobacco, non-contact sexual abuse and perpetuation of violence.
The evidence base for alcohol use among adolescents in India needs a deeper exploration. Despite gaps in the evidence base, this synthesis provides a reasonable understanding of alcohol use among adolescents in India and can provide direction to policymakers.
Introduction
According to the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019, among adolescents and young adults (aged 10–24 years), alcohol-attributable burden is second highest among all risk factors contributing to disability-adjusted life years in this age group (GBD 2019 Risk Factors Collaborators, 2020 ). The exposure of the adolescent brain to alcohol is shown to result in various cognitive and functional deficits related to verbal learning, attention, and visuospatial and memory tasks, and behavioural inefficiencies such as disinhibition and elevated risk-taking (Spear, 2018 ). Alcohol consumption in adolescents results in a range of adverse outcomes across several domains and includes road traffic accidents and other non-intentional injuries, violence, mental health problems, intentional self-harm and suicide, HIV and other infectious diseases, poor school performance and drop-out, and poor employment opportunities (Hall et al ., 2016 ).
Adolescence is a critical period in which exposure to adversities such as poverty, family conflict and negative life experiences (e.g. violence) can have long-term emotional and socio-economic consequences for adolescents, their families and communities (Knapp et al ., 1999 ; Knapp et al ., 2002 ). Substance use, including alcohol, is typically established during adolescence and this period is peak risk for onset and intensification of substance use behaviours that pose risks for short- and long-term health (Anthony and Petronis, 1995 ; DeWit et al ., 2000 ; Hallfors et al ., 2005 ; Schmid et al ., 2007 ; Hadland and Harris, 2014 ). As such, early initiation of alcohol use among adolescents can provide a useful indication of the potential future burden among adults including increased risk for academic failure, mental health problems, antisocial behaviour, physical illness, risky sexual behaviours, sexually transmitted diseases, early-onset dementia and the development of alcohol use disorders (AUDs) (Hingson et al ., 2006 ; King and Chassin, 2007 ; Dawson et al ., 2008 ; Nordström et al ., 2013 ).
India continues to develop rapidly, and accounts for most of the increase in alcohol consumption per capita for WHO's South-East Asia region (World Health Organization, 2018 ). Although India has a relatively high abstinence rate, many people who do drink are either risky drinkers or have AUDs (Benegal, 2005 ; Rehm et al ., 2009 ). Finally, the existing policies in India have failed to reduce the harm from alcohol because the implementation of alcohol control efforts is fragmented, lacks consensus, is influenced by political considerations, and is driven by narrow economic and not health concerns (Gururaj et al ., 2021 ).
India has the largest population of adolescents globally (253 million people aged 10–19 years), constituting 21% of the population (Government of India, 2011 ; Boumphrey, 2012 ). Additionally, adolescents as young as 13–15 years of age have started consuming alcohol in India (Gururaj et al ., 2016 ). Despite this growing public health problem, the official policy response in India remains primarily focused on AUDs, particularly alcohol dependence in adults, with an absolute disregard for the potential of prevention programmes. One potential reason for this is the limited understanding of the onset and progression of alcohol use and AUDs amongst adolescents in India. The aim of this paper is to bridge that knowledge gap by synthesising the evidence about the prevalence and correlates of alcohol use and AUDs in adolescents from India.
The specific objectives are to examine the following in adolescents from India: (a) prevalence of current and lifetime use of alcohol, (b) prevalence of current AUDs, (c) patterns (e.g. frequency, quantity) of alcohol use, (d) sociodemographic, social and clinical correlates of alcohol use and AUDs, and (e) explanatory models of and attitudes towards alcohol use and AUDs, e.g. perceptions of the problem and its causes. This paper synthesises the evidence about alcohol and AUDs using data from a comprehensive review that we conducted of any substance use and substance use disorders amongst adolescents in India.
Systematic review . The review protocol was registered prospectively on Prospero (registration ID CRD 42017080344).
Inclusion and exclusion criteria
There were no limits placed on the year of publication of the paper, gender of the participants and study settings in India. We only included English language publications as academic literature from India is predominantly published in such publications. Adolescents were defined as anyone between 10 and 24 years of age (Sawyer et al ., 2018 ). Studies reporting alcohol use and/or AUDs in a wider age range (including 10–24 years) were included only if data were separately presented for the 10–24-year age group. We included observational studies (surveys, case-control studies, cohort studies), qualitative studies and intervention studies (only if baseline prevalence data were presented). We included studies which examined alcohol use and AUDs defined as per the International Classification of Diseases (ICD)/Diagnostic and Statistical Manual of Mental Disorders (DSM)/clinical criteria or using a standardised screening or diagnostic tool.
We searched the following databases: PsycARTICLES, PsycInfo, Embase, Global Health, CINAHL, Medline and Indmed. The search strategy was organised under the following concepts: substance (e.g. alcohol, drug), misuse/use disorder (e.g. addiction, intoxication), young people (e.g. adolescent, child) and India (e.g. India, names of individual Indian states). The detailed search strategy is listed in Appendix A .
Two reviewers (DG and KW) independently inspected the titles and abstracts of studies identified through the database search. Any conflicts about eligibility between the two reviewers were resolved by AN. If the title and abstract did not offer enough information, the full paper was retrieved to ascertain whether it was eligible for inclusion. Screening of full texts was done by AN, AG and DG; and any conflicts about eligibility were resolved by UB. Screening of the results of the search was done using Covidence ( https://www.covidence.org/ ), an online screening and data extraction tool.
AN searched the following resources to identify relevant grey literature: Open Grey, OAlster, Google, ProQuest, official English language websites of the World Health Organization and World Bank, English language websites of ministries of each state and union territory within India responsible for substance misuse as well as the official websites of the Indian Narcotics Control Bureau and Ministry of Social Justice and Empowerment.
Any grey literature with relevant data published by a recognised non-governmental organisation, state, national or international organisation was included. Studies were included based on the robustness of study design and quality of data. If there were multiple editions of any published piece of grey literature, only the latest published edition of that report was included. Once retrieved, their titles, content pages and summaries were read by AN and if deemed eligible they were added to a list of potentially eligible reports. If the grey literature's summary, content and title did not include enough information, then the full text was examined by AN to determine eligibility for inclusion.
Finally, experts in the field of substance use disorders in India were contacted to explore if they could identify any further useful sources of information and were invited to submit unpublished data and unreported outcomes for possible inclusion into the review. Reference lists of selected studies, grey literature and relevant reviews were inspected for additional potential studies.
A formal data extraction worksheet was designed to extract data relevant to the study aims. The following data were extracted: centre (e.g. name of city), sampling technique, sample (e.g. general population), sample size, age(s), tool used to measure alcohol use and/or AUD, definitions of alcohol use and AUD, prevalence of alcohol use and/or AUD, age of initiation, type of alcohol, quantity and frequency of alcohol use, attitudes towards alcohol use, effect of alcohol on health, social, educational and other domains, and risk factors/correlates of alcohol use and or AUD. Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al ., 2015 ), a record was made of the number of papers retrieved, the number of papers excluded and the reasons for their exclusion. AT independently performed data extraction, AG checked the data extraction, and AN arbitrated any unresolved issues. The quality of reporting of included studies was examined using the STROBE Statement – checklist of items that should be included in reports of observational studies (Von Elm et al ., 2007 ).
A descriptive analysis of the data was conducted, and the results are mainly reported in a narrative format focusing on each of the objectives described above (Popay et al ., 2006 ).
In total, 6464 references were identified through the search strategies described above. Overall, 251 records were eligible for the wider review, of which 55 were about alcohol use and have been reported in this paper ( Fig. 1 ). Additionally, one report of magnitude of substance use in India which was recommended by an expert was also included (Ambekar et al ., 2019 ).

PRISMA flow diagram.
Study descriptions
One study was conducted online (Gupta et al ., 2018 ) and one in a national treatment centre in North India (Mandal et al ., 2019 ), both of which potentially had access to participants from across the country ( Table 1 ). All the rest were conducted at a single or multiple settings in a city, town, district, village or state. The sample size of the studies ranged from 23 (Bhad et al ., 2017 ) to 7350 (Jaisoorya et al ., 2016 ). In studies that reported mean age of the samples, it ranged from 13.10 years (Pillai et al ., 2008 ) to 20.56 years (Garg et al ., 2009 ).
Description of studies included in the review
Prevalence of alcohol use and AUD
The prevalence of ever use or lifetime use, broadly defined as consumption of alcohol at least once in their lifetime, ranged from 3.9% in school students aged 12–18 years (Rani and Sathiyaskaran, 2013 ) to 69.8% in 22–23-year-old medical students (Kundapur and Kodyalamoole, 2016 ) ( Table 2 ). Ever use in females ranged from 6.5% in students from class 8 to class 12 (age 12–19 years) (Jaisoorya et al ., 2016 ) to 52% in an online survey of adolescents aged 13–17 years (Gupta et al ., 2018 ), and in males it ranged from 9.79% in students from classes 9 and 11 (age up to 17 years) (Kotwal et al ., 2005 ) to 47% in an online survey of adolescents aged 13–17 years (Gupta et al ., 2018 ). The prevalence of ever use in rural areas ranged from 7.37% in high school students (Tsering et al ., 2010 ) to 20% in students aged 15–19 years (Kumar et al ., 2016 ), and in urban areas it ranged from 5.23% in high school students (Tsering et al ., 2010 ) to 23.08% in students aged 15–19 years (Kumar et al ., 2016 ).
Prevalence of alcohol use and alcohol use disorders
Current use
The definition of current use of alcohol varied across studies. The more commonly used definitions were alcohol consumption at least once in the past year for which the prevalence ranged from 10.6% in senior high school students aged 12–18 years (Mohan et al ., 1981 ) to 32.9% in 15–19-year-old individuals from rural settings (Mohan et al ., 1978b ); and at least once in the past 30 days (month) for which the prevalence ranged from 2.1% (Sharma et al ., 2015 ) in 15–19-year olds from disadvantaged urban settings and 35.6% in injectable drug users attending needle and syringe programme centres (Armstrong et al ., 2013 ). Some studies did not define current use and others used non-standard definition of current use such as ‘who had not used drugs either daily or weekly in the past month’ (27.6%) (Gupta et al ., 1987 ), and ‘habit of using alcohol, 3 days or more a week’ (0.8%) (Jayakrishnan et al ., 2016 ). The biggest countrywide survey of substance use in India reported a prevalence of current alcohol use to be 1.3% amongst those aged 10–17 years (Ambekar et al ., 2019 ).
Some studies reported the prevalence of AUDs and defined them using standardised tools (Alcohol Use Disorder Identification Test [AUDIT], CAGE questionnaire, Alcohol, Smoking and Substance Involvement Screening Test [ASSIST]), ICD 10 criteria or bespoke definitions. Among medical students (18–23 years) who were drinkers, the prevalence of hazardous drinking was 19.29% (Anandi et al ., 2018 ), alcohol dependence was 3.7–10% (Kundapur and Kodyalamoole, 2016 ; Haorongbam et al ., 2018 ), binge drinking 14–30% (Kundapur and Kodyalamoole, 2016 ; Anandi et al ., 2018 ) and ‘problem drinking’ (not defined) was 41.46% (Garg et al ., 2009 ). Among students of classes 8, 10 and 12 (12–19 years), 1.6% (2% males, 0% females) of lifetime users had alcohol dependence (Jaisoorya et al ., 2016 ). In adolescent street children (11–19 years), 37% had AUD defined as recurrent substance use resulting in one or more of the following occurring in 12 months: failure to fulfil major role obligations at work or home leads to a physically hazardous situation, or causes legal problems (Gaidhane et al ., 2008 ).
Patterns of drinking
Among drinkers, 0.6–10.4% consumed every day (Armstrong et al ., 2013 ; Jaisoorya et al ., 2016 ; Kundapur and Kodyalamoole, 2016 ), 19.1–40% consumed at least once a week (Armstrong et al ., 2013 ; Kundapur and Kodyalamoole, 2016 ), 3.8% consumed weekly (Jaisoorya et al ., 2016 ), 9.5% consumed less than once a week (Armstrong et al ., 2013 ) and 10.6% consumed monthly (Jaisoorya et al ., 2016 ) ( Table 3 ). Usual median number of drinks consumed among those between 13 and 17 years was 3.5 for both males and females (Gupta et al ., 2018 ). Among 10–19-year-old males from an urban slum over the past month, 54.2% consumed up to 50 ‘pegs’ of alcohol (Kokiwar and Jogdand, 2011 ). Among males from a low-income community, in those between 18 and 20 years, 88.2% were ‘low drinking’ (low amount/low frequency, low amount/moderate frequency or substantial amount/low frequency), 9.3% were moderate drinking (low amount/high frequency or substantial amount/moderate frequency) and 2.5% were high drinking (substantial amount/high frequency); and in those between 20 and 24 years, 82.6% were low drinking, 13.5% were moderate drinking and 3.8% were high drinking (Singh et al ., 2010 ).
Initiation of, attitudes towards, patterns of and correlates of drinking
Initiation age
The mean age for initiation of drinking ranged from 14.4 to 18.3 years ( Table 3 ). The mean age of initiation was significantly lower in rural areas compared to urban areas [10.66 ( s.d. 4.02) v . 12.5 ( s.d. 3.57); p < 0.0001] (Nagendra and Koppad, 2017 ); and locally brewed alcohol [mean ( s.d. ) 11.09 (2.775)] was initiated at a younger age compared to commercially available alcohol in an industrial town [mean ( s.d. ) 13.90 (2.194)] (Mahanta et al ., 2016 ).
Among male substance use disorder patients at drug deaddiction centres, 41.3% had initiated alcohol use between 10 and 19 years (Bashir et al ., 2015 ). Among 22–23-year-old medical students, 25.6% had started consuming alcohol between 15 and 17 years, and 10.4% had started consuming alcohol before they were 15 years (Kundapur and Kodyalamoole, 2016 ).
In students between 18 and 22 years, 18.0% had initiated drinking between 10 and 14 years, 55.1% had initiated between 15 and 19 years, and 26.9% after 19 years (Mohanty et al ., 2013 ). Among medical and dental students, 4.26% initiated before 12 years, 19.15% initiated between 12 and 18 years, and 76.60% initiated after 18 years (Rathore et al ., 2015 ). Comparing males and females, 5.88% males ( v . 0% females) initiated before 12 years, 16.18% ( v . 26.92%) initiated between 12 and 18 years, and 77.94% ( v . 73.08%) initiated after 18 years (Rathore et al ., 2015 ). Finally, comparing urban and rural drinkers, 6.50% urban drinkers ( v . 6.10% rural) initiated before 8 years, 8.94% ( v . 10.98%) initiated between 9 and 10 years, 27.65% ( v . 39.02%) initiated between 11 and 12 years, 26.83% ( v . 30.49%) initiated between 12 and 14 years, 24.39% ( v . 10.98%) initiated between 15 and 16 years, and 5.69% ( v . 2.44%) initiated after 17 years (Kumar et al ., 2016 ).
Knowledge and attitudes
Overall, 55.3% of college-going students (17–21 years) believed that there was no risk of harmful effects of alcohol; with more females than males who believed that there was no risk (69.4% v . 43.4%); and a higher proportion from villages (64.4%) thought there was no risk as compared to those from towns (60.7%) or cities (50.0%) (Kalpana and Kavya, 2012 ) ( Table 3 ). Among medical students (22–23 years), 44% considered it safe to consume alcohol, and 88% believe drinking patterns are mood-dependent (Kundapur and Kodyalamoole, 2016 ).
In medical students (17–23 years), reasons for initiation of drinking included curiosity (19.6%), attending a party (17.5%), friends' influence (15.2%) and social gatherings (9.8%); and reasons for continued use included enjoyment (31.5%), as a coping mechanism for depressive symptoms (17.8%), socialisation (14.8%) and to take mind off other issues (9.6%) (Haorongbam et al ., 2018 ). Among college-going students (mean age 16.7 years; s.d. 0.5) there was a stronger endorsement of negative reinforcements (e.g. cognitive impairment, risk taking) than of possible positive reinforcements (e.g. sociability, tension reduction); and compared to males, significantly more females felt alcohol consumption could not reduce tension and endorsed increased sociability and cognitive impairment (Sandhya et al ., 2013 ). Knowledge of harm of alcohol among substance users was greater in adolescents from urban than rural areas (61.5% v . 30.8%) (Tsering et al ., 2010 ).
Risk factors/correlates
The cross-sectional nature of the studies only allowed the examination of correlates of alcohol use ( Table 3 ). Alcohol consumption was associated with being male (Medhi et al ., 2006 ; Mohanan et al ., 2014 ; Jaisoorya et al ., 2016 ; Kundapur and Kodyalamoole, 2016 ; Anandi et al ., 2018 ; Mandal et al ., 2019 ), older age (Medhi et al ., 2006 ; Rathore et al ., 2015 ; Jaisoorya et al ., 2016 ; Gupta et al ., 2018 ; Mandal et al ., 2019 ) and going to private rather than public schools (Jain et al ., 2012 ; Rani and Sathiyaskaran, 2013 ). Specifically for locally brewed alcohol, it was associated with younger age and rural residence (Mandal et al ., 2019 ). Alcohol consumption was associated with having a part-time job, and failing a subject or a year in school (Jaisoorya et al ., 2016 ).
Alcohol use in adolescents was associated with parental/guardian's use of alcohol or tobacco, lack of parental supervision, and not having ‘understanding’ parents (Rani and Sathiyaskaran, 2013 ; Mohanan et al ., 2014 ; Jayakrishnan et al ., 2016 ; Mandal et al ., 2019 ). Alcohol use decreased with a decrease in the frequency of friends sharing alcohol-related information on Facebook and YouTube; and increased frequency of sharing personal alcohol-related content on Twitter was associated with an increase in alcohol use (Gupta et al ., 2018 ). Alcohol consumption was also associated with close friends using substances (any type) or peer pressure to drink alcohol (Mandal et al ., 2019 ).
Alcohol consumption was associated with tobacco use, illicit drug use, attention deficit hyperactivity disorder (ADHD) symptoms, suicidal thinking, planning and attempts, and non-contact sexual abuse and perpetuation of violence (Nadkarni et al ., 2015 ; Jaisoorya et al ., 2016 ). Finally, higher acceptance of alcohol is associated with lower spirituality, less religiosity, less ‘God Consciousness’ and less formal religious practices (Sukhwal and Suman, 2013 ).
Quality of reporting studies
In 42 of the 57 studies, there was appropriate reporting of more than 70% of the 22 STROBE criteria ( Appendix B ). Only one study reported on all the 22 criteria (Nadkarni et al ., 2015 ). For 15 of the 22 criteria, there was appropriate reporting in more than 70% of the studies. The poorest reporting was about study biases, generalisability of the findings, and role of the funder.
The existing evidence base has several limitations which preclude a robust synthesis and any conclusions we draw are, at best, exploratory in nature. Although the information about AUDs is relatively limited, the prevalence among drinkers appears to be high, and the patterns of drinking in a reasonably high proportion were suggestive of risky drinking (heavy drinking that puts the drinker at risk of developing problems), especially considering that this is a young population with a relatively short drinking history.
This is consistent with the steady rise in recorded alcohol consumption in most developing countries, albeit from relatively low base prevalence rates. It also parallels the increases in adult per capita consumption of alcohol and heavy episodic drinking that have been observed in India and other developing economies in east Asia, south Asia and southeast Asia (Shield et al ., 2020 ). Amongst adolescents, the prevalence of current alcohol use in Sri Lanka was 3.4% (95% CI 2.6–4.3) (Senanayake et al ., 2018 ), lifetime alcohol use in males was 45% (26% risky drinking) in Pakistan (Shahzad et al ., 2020 ), alcohol use was reported by 19% from traditional non-alcohol using ethnic groups and 40% from traditional alcohol using ethnic groups in Nepal (Parajuli et al ., 2015 ), and 13% in Bhutan (Norbu and Perngparn, 2014 ).
The data about patterns of drinking observed among adolescents in India are inconclusive but there appears to be some tendency towards heavy drinking. Among adolescents across several countries, there are consistent reports of binge drinking as a social norm among peer groups (Russell-Bennett et al ., 2010 ). The prevalence of binge drinking increases from age 15–19 years to the age of 20–24 years, and among drinkers, binge drinking is higher among the 15–19 years age group compared with the total population of drinkers (World Health Organization, 2018 ). This means that 15–24-year-old current drinkers often drink in heavy drinking sessions, and hence, except for the Eastern Mediterranean Region, the prevalence of such drinking among drinkers is high in adolescents (around 45–55%) (World Health Organization, 2018 ).
In India, the age of initiation commonly was mid- to late-teens; and male gender, rural residence and locally brewed alcohol were associated with earlier initiation of drinking. Across most of the world, initiation of alcohol use among adolescents takes place at an early age, usually before the age of 15 years. Among 15-year-olds, there is a high prevalence of alcohol use (50–70%) during the past 30 days in many countries of the Americas, Europe and Western Pacific; and the prevalence is relatively lower in African countries (10–30%) (World Health Organization, 2018 ). However, across the world, there is a huge variation in alcohol use among boys and girls of 15 years of age and vary from 1.2% to 74.0% in boys and 0% to 73.0% in girls (World Health Organization, 2018 ). Finally, with the strategic targeting of adolescents as alcohol consumers by the industry, increasing overall population prevalence and normalisation of drinking alcohol, and the increasing normalisation by virtue of learning more about how adolescents in other countries drink, one could speculate that the age of initiation would reduce and prevalence of alcohol consumption in adolescents in India would rise, in the coming years.
In India, knowledge about alcohol and its potential harms was limited in rural areas. The reasons for starting and continuing drinking were a mix of expected enhancement of positive experiences and dampening of negative affect. This is consistent with findings in Indian adults where alcohol consumption was seen to be mainly associated with expectations about reduction in psychosocial stress and providing pleasure (Nadkarni et al ., 2013 ). Across the world, adolescents primarily report drinking for social motives or enjoyment – enjoyment (Argentina) (Jerez and Coviello, 1998 ), to make nights out more pleasurable (UK) (Plant et al ., 1990 ) and being social (Canada) (Kairouz et al ., 2002 ). Coping motives, on the other hand, are less common, but are associated with AUDs later in adulthood (Carpenter and Hasin, 1999 ). The difference in drinking motives between adolescents from India (a mix of pleasure and coping) and other countries (primarily pleasure), and the similarity between reasons given by Indian adolescents and Indian adults, possibly reflect contextual/cultural differences and will have implications on transferability of interventions from other contexts and wider age-applicability of interventions developed for adults in India.
We can broadly organise our findings about correlates for drinking into socio-demographic characteristics (e.g. age, gender), immediate environment (e.g. parents, friends, digital space) and clinical correlates (e.g. other substance use, suicidal thoughts). Risk and protective factors influencing the use of alcohol in adolescents are both proximal and distal factors and include individual cognitions and peer-influence risk factors (e.g. attitudes favourable to alcohol use and peer drinking), family environment (e.g. parental discipline and family bonding) and school context (e.g. academic commitment and achievement) (Bryant et al ., 2003 ; Fisher et al ., 2007 ; Patock-Peckham and Morgan-Lopez, 2010 ). Most commonly adolescent males drink more often than adolescent females, but there has been some blurring of the distinction between the genders in developed countries (Currie et al ., 2004 ; Hibell et al ., 2009 ). This convergence of drinking patterns is particularly seen in the Nordic countries, Ireland, the UK and the USA, and manifests as almost equal prevalence rates for consumption of spirits and similar frequency of intoxication for both genders (Hibell et al ., 2009 ). Evidence from South Asian countries indicates that male gender, age greater than 14 years, depression, religious beliefs, parental/family members' drinking, reduced parental supervision, peer-drinking/pressure/approval and urban neighbourhood are associated with adolescent drinking (Athauda et al ., 2020 ).
The most important study finding is that despite several studies over the years, the evidence base has several gaps, notably the limited geographical span, small sample sizes and heterogeneous definitions of alcohol use and AUDs. Of particular importance are the various sample selection strategies, especially for the smaller studies, which limit the generalisability of findings. Another gap is the lack of consistency in the measurement of alcohol use, which is especially critical in a context where ‘standard drink’ does not translate semantically or literally into the vernacular, and there is an immense variability in the types of alcoholic beverages (commercial, licit non-commercial, illicit home-brewed, adulterated alcoholic beverages) and in the type and size of vessels from which alcohol is poured or consumed in. Additionally, there were several gaps in the reporting of many studies which raise questions about their internal validity. In the absence of critical information such as data sources, measurement and statistical methods, it is difficult to draw an inference about the robustness of the studies which had inadequate reporting ( Appendix B ). Finally, although the cross-sectional design of the studies allows us to examine the prevalence of alcohol use and AUDs, it limits the conclusions that we can draw about causal relationships between the various potential risk factors and alcohol use/AUDs.
Although the included studies are not without limitations that are important to consider before drawing conclusions, this synthesis allows us to get a reasonable understanding of alcohol use among adolescents in India and derive preliminary conclusions that the prevalence is high and rising, which brings with it the attendant burden of the associated adverse impacts. Furthermore, despite the gaps in the available data, it carries several implications for policy makers. Because alcohol is an important cause of motor vehicle accidents and suicide, which are the leading causes of death among adolescents in India (Joshi et al ., 2017 ), interventions that seek to help adolescents avoid or better manage alcohol consumption are a priority. Examples of such evidence-based interventions include public health engagement campaigns to increase awareness of alcohol-related harms, advocacy through community engagement/mobilisation to promote better enforcement of laws related to drinking, engagement with alcohol outlets to promote responsible beverage service, and engaging adolescents and families including through peer-led classroom curriculum to enhance the resilience of adolescents, improve family socialisation and increase awareness of alcohol-related harms (McLeroy et al ., 2003 ; Hawkins et al ., 2008 ; Wakefield, Loken, and Hornik, 2010 ; Hallgren and Andréasson, 2013 ). The most important implication of our review, however, is the need to develop the very nascent literature base through robust studies, especially longitudinal research that can support evidence-based prevention interventions and policy change. Future studies should focus on increasing their geographical span and sample sizes, ensure the use of standard definitions of alcohol use and AUDs which are consistent with global literature, and acknowledge and examine contextual variations in types of alcoholic beverages and type and size of vessels from which alcohol is poured or consumed in. Introducing such measures will enhance the robustness, validity and generalisability of the findings; and allow for better comparisons over time and geography. This would require greater support from the Government through ensuring availability of in-country research funding, prioritisation of the issue and utilisation of the evidence generated to inform its policy on alcohol.
Our review is limited by our inclusion criterion related to language. However, this might not be a major limitation considering that peer-reviewed journals in India are only in English as far as we are aware, and researchers generally disseminate their outputs in English language journals. Our review's major strength lies in its originality (the first such review to comprehensively map the landscape of substance use among adolescents in India), use of robust processes (e.g. double screening) and examination of grey literature to identify any relevant evidence.
To conclude, the evidence base for alcohol use amongst adolescents in India needs further and deeper exploration, but in the meanwhile, the available evidence allows us to get a preliminary understanding of the issue and to make a case for policy action to tackle alcohol consumption in this age group.
Acknowledgements
We would like to acknowledge Professor Pratima Murthy, Professor Vivek Benegal and Professor Atul Ambekar for helping us identify relevant grey literature.
Appendix A: Search strategy
- disorders.tw
- withdraw*.tw
- withdrawal syndrome.tw
- withdrawal syndrome/
- screening.tw
- overdose.tw
- megadose.tw
- dependen*.tw
- intoxication.tw
- intoxication/
- behavior.tw
- alcoholi*.tw
- delirium.tw
- binge drink*.tw
- binge drink*/
- consumption.tw
- consumption/
- cessation.tw
- OR (1–50)
- Substance.tw
- ‘purple drank’.tw
- ‘purple drank’/
- unclassified drug.tw
- unclassified drug/
- chlorobenzoic acid derivative.tw
- chlorobenzoic acid derivative/
- methadone.tw
- morphine.tw
- buprenorphine.tw
- buprenorphine/
- diamorphine.tw
- diamorphine/
- amphetamine.tw
- amphetamine/
- amphetamine derivative.tw
- amphetamine derivative/
- cigarette.tw
- electronic cigarette.tw
- electronic cigarette/
- benzodiazepine derivative.tw
- benzodiazepine derivative/
- benzodiazepine.tw
- benzodiazepine/
- cannabi*.tw
- ‘brown sugar’.tw
- ‘brown sugar’/
- medical cannabi*.tw
- medical cannabi*/
- tetrahydrocannabinol.tw
- tetrahydrocannabinol/
- cocaine derivative.tw
- cocaine derivative/
- chlorpheniramine.tw
- chlorpheniramine/
- ‘cough syrup’.tw
- ‘cough syrup’/
- dexamphetamine.tw
- dexamphetamine/
- dextromethorphan.tw
- dextromethorphan/
- 3,4 methylenedioxyamphetamine.tw
- 3,4 methylenedioxyamphetamine/
- psychedelic agent.tw
- psychedelic agent/
- 4 aminobutyric acid.tw
- 4 aminobutyric acid/
- 4 hydroxybutyric acid.tw
- 4 hydroxybutyric acid/
- Ketamine.tw
- nicotine.tw
- inhalant.tw
- kava extract.tw
- kava extract/
- smokeless tobacco.tw
- smokeless tobacco/
- laughing gas.tw
- laughing gas/
- nitrous oxide.tw
- nitrous oxide/
- Lysergic acid diethylamide.tw
- Lysergic acid diethylamide/
- magic mushroom.tw
- magic mushroom/
- hallucinogenic fungus.tw
- hallucinogenic fungus/
- mari#uana.tw
- Midomafetamine.tw
- Midomafetamine/
- methamphetamine.tw
- Methamphetamine/
- Crystal meth.tw
- Crystal meth/
- Amobarbital.tw
- Amobarbital/
- Methylphenidate.tw
- Methylphenidate/
- Modafinil.tw
- Morphine.tw
- ‘paint thinner’.tw
- ‘paint thinner’/
- promethazine.tw
- promethazine/
- psilocybin#.tw
- psilocybin#/
- Quaalude.tw
- Methaqualone.tw
- Methaqualone/
- Salvia divinorum.tw
- Salvia divinorum/
- Psychotropic agent.tw
- Psychotropic agent/
- Chewing tobacco.tw
- Chewing tobacco/
- Tramadol.tw
- Sildenafil.tw
- Sildenafil/
- Eszopiclone.tw
- Eszopiclone/
- Zaleplon.tw
- Zoipidem.tw
- Zopiclone.tw
- Hypnotic agent.tw
- Hypnotic agent/
- Prescription durg.tw
- Prescription drug/
- Prescription medicine.tw
- Prescription medicine/
- Prescription medication.tw
- Prescription medication/
- OR (52-255)
- adolescen*.tw
- adolescen*/
- student*.tw
- young adult*.tw
- young adult*/
- OR (257-274)
- ‘Indian union’.tw
- ‘Indian union’/
- Andaman and Nicobar Island*.tw
- Andaman and Nicobar Island/
- Andhra Pradesh.tw
- Andhra Pradesh/
- Arunachal Pradesh.tw
- Arunachal Pradesh/
- Dadra and Nagar Haveli.tw
- Dadra and Nagar Haveli/
- Chhattisgarh.tw
- Chhattisgarh/
- Daman and Diu.tw
- Daman and Diu/
- National Capital Territory of New Delhi.tw
- National Capital Territory of New Delhi/
- Himachal Pradesh.tw
- Himachal Pradesh/
- Jammu and Kashmir.tw
- Janmu and Kashmir/
- Jharkhand.tw
- Karnataka.tw
- Travancore-Cochin.tw
- Travancore-Cochin/
- Madhya Pradesh.tw
- Madhya Pradesh/
- Madhya Bharat.tw
- Madhya Bharat/
- Maharashtra.tw
- Maharashtra/
- Meghalaya.tw
- Nagaland.tw
- Chandigarh.tw
- Chandigarh/
- Rajasthan.tw
- Tamil Nadu.tw
- Tamil Nadu/
- Madras State.tw
- Madras State/
- Telangana.tw
- Uttarakhand.tw
- Uttarakhand/
- Uttaranchal.tw
- Uttaranchal/
- Uttar Pradesh.tw
- Uttar Pradesh/
- United Provinces.tw
- United Provinces/
- West Bengal.tw
- West Bengal/
- Lakshadweep.tw
- Lakshadweep/
- P#d#cherry.tw
- P#d#cherry/
- OR (276–375)
- 51 AND 256 AND
Appendix B: Quality of reporting of peer-reviewed studies included in the review (excluding the report)
Supplementary material, financial support.
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Conflict of interest
There are no real or perceived conflicts of interest in undertaking or publishing this research.
Ethical standards
As this is a systematic review, it did not involve any direct data collection from human subjects.
- Ahmad A, Khalique N and Khan Z (2009) Analysis of substance abuse in male adolescents . Iran Journal of Pediatrics 19 , 399–403. [ Google Scholar ]
- Ambekar A, Agrawal A, Rao R, Mishra AK, Khandelwal SK, Chadda RK and on behalf of the group of investigators for the National Survey on Extent and Pattern of Substance Use in India (2019) Magnitude of Substance Use in India . New Delhi: Ministry of Social Justice and Empowerment, Government of India. [ Google Scholar ]
- Anandi BS, Halgar PK, Reddy SB and Indupalli AS (2018) A cross-sectional study to assess the prevalence of harmful alcohol consumption habits among students of a medical college . Community Medicine 9 , 719–724. [ Google Scholar ]
- Anthony JC and Petronis KR (1995) Early-onset drug use and risk of later drug problems . Drug and Alcohol Dependence 40 , 9–15. [ PubMed ] [ Google Scholar ]
- Armstrong G, Nuken A, Samson L, Singh S, Jorm AF and Kermode M (2013) Quality of life, depression, anxiety, and suicidal ideation among men who inject drugs in Delhi, India . BMC Psychiatry 13 , 151. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Arya S, Gupta R, Rathee S and Rawat V (2016) Immediate drop-out rate in adolescent substance abusers: an out-patient chart review from North India . International Journal of Adolescent Medicine and Health 29 . 20160020. [ PubMed ] [ Google Scholar ]
- Athauda LK, Peiris-John R, Ameratunga S, McCool J and Wickremasinghe R (2020) Factors influencing alcohol use among adolescents in south Asia: a systematic review . Journal of Studies on Alcohol and Drugs 81 , 529–542. [ PubMed ] [ Google Scholar ]
- Bahl R and Kumari R (2016) Mental health profile of urban and rural adolescents in Jammu district of J&K . JK Science 18 , 221–224. [ Google Scholar ]
- Bardhan T, Saikia AM and Baruah R (2015) Substance use among adolescents living in slums of Guwahati city, Assam: a growing public health concern . International Journal of Medicine and Public Health 5 , 279–282. [ Google Scholar ]
- Bashir N, Sheikh AA, Bilques S and Firdosi MM (2015) Socio-demographic correlates of substance use disorder patients seeking de-addiction services in Kashmir India – a cross sectional study . British Journal of Medical Practitioners 8 , a833–a833. [ Google Scholar ]
- Benegal V (2005) India: alcohol and public health . Addiction 100 , 1051–1056. [ PubMed ] [ Google Scholar ]
- Bhad R, Jain R, Dhawan A and Mehta M (2017) A clinic-based study in treatment-seeking adolescent inhalant users in India: implications for management . Journal of Child & Adolescent Substance Abuse 26 , 91–101. [ Google Scholar ]
- Boumphrey S (2012) Special Report: The World's Youngest Populations . Retrieved from http://blog.euromonitor.com/2012/02/special-report-the-worlds-youngest- populations-.html.
- Bryant AL, Schulenberg JE, O'Malley PM, Bachman JG and Johnston LD (2003) How academic achievement, attitudes, and behaviors relate to the course of substance use during adolescence: a 6-year, multiwave national longitudinal study . Journal of Research on Adolescence 13 , 361–397. [ Google Scholar ]
- Carpenter KM and Hasin DS (1999) Drinking to cope with negative affect and DSM-IV alcohol use disorders: a test of three alternative explanations . Journal of Studies on Alcohol 60 , 694–704. [ PubMed ] [ Google Scholar ]
- Currie C, Roberts C, Settertobulte W, Morgan A, Smith R and Samdal O (2004) Young People's Health in Context: Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2001/2002 Survey . Copenhagen: WHO Regional Office for Europe. [ Google Scholar ]
- Dawson DA, Goldstein RB, Patricia Chou S, June Ruan W and Grant BF (2008) Age at first drink and the first incidence of adult-onset DSM-IV alcohol use disorders . Alcoholism: Clinical and Experimental Research 32 , 2149–2160. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Deb R, Saxena S and Dubey A (2013) Trends of smoking among the youth of Delhi . South Asian Anthropologist 13 , 43–44. [ Google Scholar ]
- DeWit DJ, Adlaf EM, Offord DR and Ogborne AC (2000) Age at first alcohol use: a risk factor for the development of alcohol disorders . American Journal of Psychiatry 157 , 745–750. [ PubMed ] [ Google Scholar ]
- Fisher LB, Miles IW, Austin SB, Camargo CA and Colditz GA (2007) Predictors of initiation of alcohol use among US adolescents: findings from a prospective cohort study . Archives of Pediatrics & Adolescent Medicine 161 , 959–966. [ PubMed ] [ Google Scholar ]
- Gaidhane AM, Syed Zahiruddin Q, Waghmare L, Shanbhag S, Zodpey S and Joharapurkar SR (2008) Substance abuse among street children in Mumbai . Vulnerable Children and Youth Studies 3 , 42–51. [ Google Scholar ]
- Garg A, Chavan B, Singh G and Bansal E (2009) Patterns of alcohol consumption in medical students . Journal of the Indian Medical Association 107 , 154–155. [ PubMed ] [ Google Scholar ]
- Government of India (2011) Census of India 2011. Retrieved 18th November 2017, from Government of India. http://censusindia.gov.in/2011census/censusinfodashboard/stock/profiles/en/IND0 30_Goa.pdf.
- Gupta R, Narang R, Verma S, Panda JK, Garg D, Munjal A and Singh S (1987) Drug abuse among non-student youth labour . Indian Journal of Psychiatry 29 , 359. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Gupta H, Lam T, Pettigrew S and Tait RJ (2018) The association between exposure to social media alcohol marketing and youth alcohol use behaviors in India and Australia . BMC Public Health 18 , 726. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Gururaj G, Varghese M, Benegal V, Rao G, Pathak K, Singh L and Singh RL (2016) National Mental Health Survey of India, 2015–16: Summary. Bengaluru, National Institute of Mental Health and Neuro Sciences, NIMHANS Publication (128).
- Gururaj G, Gautham MS and Arvind BA (2021) Alcohol consumption in India: a rising burden and a fractured response . Drug and Alcohol Review 40 , 368–384. [ PubMed ] [ Google Scholar ]
- Hadland SE and Harris SK (2014) Youth marijuana use: state of the science for the practicing clinician . Current Opinion in Pediatrics 26 , 420. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Hall WD, Patton G, Stockings E, Weier M, Lynskey M, Morley KI and Degenhardt L (2016) Why young people's substance use matters for global health . The Lancet. Psychiatry 3 , 265–279. [ PubMed ] [ Google Scholar ]
- Hallfors DD, Waller MW, Bauer D, Ford CA and Halpern CT (2005) Which comes first in adolescence – sex and drugs or depression? American Journal of Preventive Medicine 29 , 163–170. [ PubMed ] [ Google Scholar ]
- Hallgren M and Andréasson S (2013) The Swedish six-community alcohol and drug prevention trial: effects on youth drinking . Drug Alcohol Review 32 , 504–511. [ PubMed ] [ Google Scholar ]
- Haorongbam M, Sathyanarayana M and Dhanashree A (2018) Depression and alcohol use in undergraduate medical students in a private medical college . Journal of Evolution of Medical and Dental Sciences 7 , 1473–1480. [ Google Scholar ]
- Hawkins JD, Brown EC, Oesterle S, Arthur MW, Abbott RD and Catalano RF (2008) Early effects of communities that care on targeted risks and initiation of delinquent behavior and substance use . Journal of Adolescent Health 43 , 15–22. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Hibell B, Guttormsson U, Ahlström S, Balakireva O, Bjarnason T, Kokkevi A and Kraus L (2009) The 2007 ESPAD Report. Substance Use Among Students in 35 European Countries . Stockholm: The Swedish Council for Information on Alcohol and Other Drugs.
- Hingson RW, Heeren T and Winter MR (2006) Age at drinking onset and alcohol dependence: age at onset, duration, and severity . Archives of Pediatrics & Adolescent Medicine 160 , 739–746. [ PubMed ] [ Google Scholar ]
- Jain A, Dhanawat J, Kotian MS and Angeline R (2012) Assessment of risk factors of non-communicable diseases among high school students in Mangalore. India . International Journal of Health & Allied Sciences 1 , 249. [ Google Scholar ]
- Jaisoorya T, Beena K, Beena M, Ellangovan K, Jose DC, Thennarasu K and Benegal V (2016) Prevalence and correlates of alcohol use among adolescents attending school in Kerala, India . Drug and Alcohol Review 35 , 523–529. [ PubMed ] [ Google Scholar ]
- Jayakrishnan R, Geetha S, Binukumarm B and Sreekumarm KL (2011) Self-reported tobacco use, knowledge on tobacco legislation and tobacco hazards among adolescents in rural Kerala State . Indian Journal of Dental Research 22 , 195. [ PubMed ] [ Google Scholar ]
- Jayakrishnan R, Geetha S, Mohanan Nair JKKP, Thomas G and Sebastian P (2016) Tobacco and alcohol use and the impact of school based antitobacco education for knowledge enhancement among adolescent students of rural Kerala, India . Journal of Addiction 2016 , 9570517. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Jerez SJ and Coviello A (1998) Alcohol drinking and blood pressure among adolescents . Alcohol 16 , 1–5. [ PubMed ] [ Google Scholar ]
- Joshi R, Alim M, Maulik PK and Norton R (2017) A contemporary picture of the burden of death and disability in Indian adolescents: data from the Global Burden of Disease Study . International Journal of Epidemiology 46 , 2036–2043. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Kairouz S, Gliksman L, Demers A and Adlaf EM (2002) For all these reasons, I do…drink: a multilevel analysis of contextual reasons for drinking among Canadian undergraduates . Journal of Studies on Alcohol 63 , 600–608. [ PubMed ] [ Google Scholar ]
- Kalpana L and Kavya HG (2012) Knowledge towards ATOD (alcohol, tobacco and other drugs): a study . Journal of Clinical and Diagnostic Research 6 , 38–41. [ Google Scholar ]
- Katyal R, Bansal R, Agrawal V, Goel K and Chaudhary V (2014) Cross-sectional study to acknowledge the independent association of the socio-demographic determinants of alcohol use in an urban slum of North India . International Journal of Preventive Medicine 5 , 749. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- King KM and Chassin L (2007) A prospective study of the effects of age of initiation of alcohol and drug use on young adult substance dependence* . Journal of Studies on Alcohol and Drugs 68 , 256–265. [ PubMed ] [ Google Scholar ]
- Knapp M, Scott S and Davies J (1999) The cost of antisocial behaviour in younger children . Clinical Child Psychology and Psychiatry 4 , 457–473. [ Google Scholar ]
- Knapp M, McCRONE P, Fombonne E, Beecham J and Wostear G (2002) The Maudsley long-term follow-up of child and adolescent depression . The British Journal of Psychiatry 180 , 19–23. [ PubMed ] [ Google Scholar ]
- Kokiwar PR and Jogdand GRS (2011) Prevalence of substance use among male adolescents in an urban slum area of Karimnagar district, Andhra Pradesh . Indian Journal of Public Health 55 , 42. [ PubMed ] [ Google Scholar ]
- Kotwal A, Thakur R and Seth T (2005) Correlates of tobacco-use pattern amongst adolescents in two schools of New Delhi, India . Indian Journal of Medical Sciences 59 , 243–252. [ PubMed ] [ Google Scholar ]
- Kumar V, Kumar D, Shora TN, Dewan D, Mengi V and Razaq M (2016) Prevalence of tobacco, alcohol, and other drug abuse among school-going male adolescents in Jammu . International Journal of Medical Science and Public Health 1 , 246–251. [ Google Scholar ]
- Kundapur R and Kodyalamoole NK (2016) Patterns in consumption of alcohol among medical interns in Mangalore, South India . Indian Journal of Public Health Research & Development 7 , 136–140. [ Google Scholar ]
- Lal B and Singh G (1979) Drug abuse in Punjab . British Journal of Addiction 74 , 411–427. [ PubMed ] [ Google Scholar ]
- Mahanta B, Mohapatra P, Phukan N and Mahanta J (2016) Alcohol use among school-going adolescent boys and girls in an industrial town of Assam, India . Indian Journal of Psychiatry 58 , 157–163. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Mandal P, Parmar A, Ambekar A and Dhawan A (2019) Substance use among treatment seeking Indian adolescent girls: are they unique? Asian Journal of Psychiatry 41 , 17–19. [ PubMed ] [ Google Scholar ]
- McLeroy KR, Norton BL, Kegler MC, Burdine JN and Sumaya CV (2003) Community-based interventions . American Journal of Public Health 93 , 529–533. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Medhi G, Hazarika N and Mahanta J (2006) Tobacco and alcohol use among the youth of the agricultural tea industry in Assam, India . Southeast Asian Journal of Tropical Medicine and Public Health 37 , 581. [ PubMed ] [ Google Scholar ]
- Meshram II, Gade S and Battina P (2015) Nutritional status and substance abuse among street children in South India . Indian Journal of Community Health 27 , 52–59. [ Google Scholar ]
- Mohan D and Arora A (1976) Prevalence and pattern of drug abuse among Delhi University college students . Journal of the Indian Medical Association 66 , 28–33. [ PubMed ] [ Google Scholar ]
- Mohan D, Prabhakar A, Mohun M and Chitkara B (1978a) Factors associated with the prevalence of drug abuse among Delhi University students . Indian Journal of Psychiatry 20 , 332–338. [ Google Scholar ]
- Mohan D, Sharma HK, Darshan S, Sundaram KR and Neki JS (1978b) Prevalence of drug abuse in young rural males in Punjab . Indian Journal of Medical Research 68 , 689–694. [ PubMed ] [ Google Scholar ]
- Mohan D, Rustagi P, Sundaram K and Prabhu G (1981) Relative risk of adolescent drug abuse: Part I socio-demographic and interpersonal variables . Bulletin on Narcotics 33 , 1–8. [ PubMed ] [ Google Scholar ]
- Mohanan P, Swain S, Sanah N, Sharma V and Ghosh D (2014) A study on the prevalence of alcohol consumption, tobacco use and sexual behaviour among adolescents in urban areas of the Udupi District, Karnataka, India . Sultan Qaboos University Medical Journal 14 , e104. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Mohanty S, Tripathy R, Palo SK and Jena D (2013) Socioeconomic, demographic study on substance abuse among students of professional college in a southern town, Berhampur of Odisha state (India) . Journal of Forensic and Legal Medicine 20 , 1057–1062. [ PubMed ] [ Google Scholar ]
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A and Petticrew M (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement . Systematic Reviews 4 , 1. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- GBD 2019 Risk Factors Collaborators (2020) Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019 . Lancet (London, England) 396 , 1223–1249. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Nadkarni A, Dabholkar H, McCambridge J, Bhat B, Kumar S, Mohanraj R and Patel V (2013) The explanatory models and coping strategies for alcohol use disorders: an exploratory qualitative study from India . Asian Journal of Psychiatry 6 , 521–527. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Nadkarni A, Dean K, Weiss HA and Patel V (2015) Prevalence and correlates of perpetration of violence among young people: a population-based survey from Goa, India . Asia Pacific Journal of Public Health 27 , NP2512–NP2520. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Nagendra K and Koppad R (2017) Prevalence of health risk behaviours among adolescents of Shivamogga: a cross-sectional study . National Journal of Community Medicine 8 , 33–36. [ Google Scholar ]
- Naik PR, Gokhe SSB, Shinde RR and Nirgude AS (2011) Street children of Mumbai: demographic profile and substance abuse . Biomedical Research 22 , 495–498. [ Google Scholar ]
- Ningombam S, Hutin Y and Murhekar MV (2011) Prevalence and pattern of substance use among the higher secondary school students of Imphal, Manipur, India . The National Medical Journal of India 24 , 11–15. [ PubMed ] [ Google Scholar ]
- Norbu T and Perngparn U (2014) Drugs and alcohol use by secondary school students in Thimphu, Bhutan . Journal of Health Research 28 , 173–182. [ Google Scholar ]
- Nordström P, Nordström A, Eriksson M, Wahlund L-O and Gustafson Y (2013) Risk factors in late adolescence for young-onset dementia in men: a nationwide cohort study risk factors for young-onset dementia in men risk factors for young-onset dementia in men . JAMA Internal Medicine 173 , 1612–1618. [ PubMed ] [ Google Scholar ]
- Nuken A, Kermode M, Saggurti N, Armstrong G and Medhi GK (2013) Alcohol and condom use among HIV-positive and HIV-negative female sex workers in Nagaland, India . International Journal of STD & AIDS 24 , 695–702. [ PubMed ] [ Google Scholar ]
- Olumide AO, Robinson AC, Levy PA, Mashimbye L, Brahmbhatt H, Lian Q and Blum RW (2014) Predictors of substance use among vulnerable adolescents in five cities: findings from the well-being of adolescents in vulnerable environments study . Journal of Adolescent Health 55 , S39–S47. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Parajuli VJ, Macdonald S and Jimba M (2015) Social–contextual factors associated with alcohol use among adolescents of traditional alcohol user and nonuser ethnic groups of Nepal . Journal of Ethnicity in Substance Abuse 14 , 151–165. [ PubMed ] [ Google Scholar ]
- Patock-Peckham JA and Morgan-Lopez AA (2010) Direct and mediational links between parental bonds and neglect, antisocial personality, reasons for drinking, alcohol use, and alcohol problems . Journal of Studies on Alcohol and Drugs 71 , 95–104. [ PubMed ] [ Google Scholar ]
- Pillai A, Patel V, Cardozo P, Goodman R, Weiss HA and Andrew G (2008) Non- traditional lifestyles and prevalence of mental disorders in adolescents in Goa, India . The British Journal of Psychiatry 192 , 45–51. [ PubMed ] [ Google Scholar ]
- Pillai A, Andrews T and Patel V (2009) Violence, psychological distress, and the risk of suicidal behaviour in young people in India . International Journal of Epidemiology 38 , 459–469. [ PubMed ] [ Google Scholar ]
- Plant MA, Bagnall G and Foster J (1990) Teenage heavy drinkers: alcohol-related knowledge, beliefs, experiences, motivation, and the social context of drinking . Alcohol and Alcoholism 25 , 691–698. [ PubMed ] [ Google Scholar ]
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M and Duffy S (2006) Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC methods programme Version 1, b92.
- Rani MA and Sathiyaskaran B (2013) Mental health symptoms and substance use among urban school going adolescents . Journal of Indian Association for Child & Adolescent Mental Health 9 , 102–135. [ Google Scholar ]
- Rathore M, Pankaj J, Mangal A and Saini P (2015) Study of alcohol use among undergraduate medical and dental students of a private medical university in Rajasthan . International Journal of Medical and Health Sciences 4 , 369–376. [ Google Scholar ]
- Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y and Patra J (2009) Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders . The Lancet 373 , 2223–2233. [ PubMed ] [ Google Scholar ]
- Russell-Bennett R, Hogan S and Perks K (2010). A qualitative investigation of socio-cultural factors influencing binge-drinking: a multi-cultural study. Paper presented at the Proceedings of the Australian and New Zealand Marketing Academy Conference 2010 .
- Sandhya B, Carol B, Kotian M and Ganaraja B (2013) Alcohol expectancy responses from teenagers: the early forewarning signals . Journal of Clinical and Diagnostic Research 7 , 489. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Sarangi L, Acharya HP and Panigrahi OP (2008) Substance abuse among adolescents in urban slums of Sambalpur . Indian Journal of Community Medicine 33 , 265. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Sawyer SM, Azzopardi PS, Wickremarathne D and Patton GC (2018) The age of adolescence . The Lancet Child Adolescent Health 2 , 223–228. [ PubMed ] [ Google Scholar ]
- Saxena V, Saxena Y, Kishore G and Kumar P (2010) A study on substance abuse among school going male adolescents of Doiwala Block, District Dehradun . Indian Journal of Public Health 54 , 197. [ PubMed ] [ Google Scholar ]
- Schmid B, Hohm E, Blomeyer D, Zimmermann US, Schmidt MH, Esser G and Laucht M (2007) Concurrent alcohol and tobacco use during early adolescence characterizes a group at risk . Alcohol and Alcoholism 42 , 219–225. [ PubMed ] [ Google Scholar ]
- Senanayake S, Gunawardena S, Kumbukage M, Wickramasnghe C, Gunawardena N, Lokubalasooriya A and Peiris R (2018) Smoking, alcohol consumption, and illegal substance abuse among adolescents in Sri Lanka: results from Sri Lankan global school-based health survey 2016 . Advances in Public Health 2018 . 9724176. [ Google Scholar ]
- Shahzad S, Kliewer W, Ali M and Begum N (2020) Different risk factors are associated with alcohol use versus problematic use in male Pakistani adolescents . International Journal of Psychology 55 , 585–589. [ PubMed ] [ Google Scholar ]
- Sharma S, Singh M, Lal P and Goel S (2015) Predictors of tobacco use among youth in India: GATS 2009–2010 survey . Asian Pacific Journal of Cancer Prevention 16 , 7535–7540. [ PubMed ] [ Google Scholar ]
- Sharma S, Sharma G and Barkataki B (2016) Substance use and criminality among juveniles-under-enquiry in New Delhi . Indian Journal of Psychiatry 58 , 178–182. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Shield K, Manthey J, Rylett M, Probst C, Wettlaufer A, Parry CD and Rehm J (2020) National, regional, and global burdens of disease from 2000 to 2016 attributable to alcohol use: a comparative risk assessment study . The Lancet Public Health 5 , e51–e61. [ PubMed ] [ Google Scholar ]
- Shrivastava SRB and Bobhate PS (2010) Tobacco quit rates among youth in an urban health centre of Mumbai: a cross sectional study . Addiction & Health 2 , 111. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Singh S and Preet K (1981) Drug abuse amongst school and college students in Punjab . Child Psychiatry Quarterly 14 , 5–11. [ Google Scholar ]
- Singh S, Schensul JJ, Gupta K, Maharana B, Kremelberg D and Berg M (2010) Determinants of alcohol use, risky sexual behavior, and sexual health problems among men in low-income communities of Mumbai, India . AIDS and Behavior 14 , 48–60. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Spear LP (2018) Effects of adolescent alcohol consumption on the brain and behaviour . Nature Reviews Neuroscience 19 , 197–214. [ PubMed ] [ Google Scholar ]
- Sukhwal M and Suman L (2013) Spirituality, religiosity, and alcohol related beliefs among college students . Asian Journal of Psychiatry 6 , 66–70. [ PubMed ] [ Google Scholar ]
- Tsering D, Pal R and Dasgupta A (2010) Licit and illicit substance use by adolescent students in eastern India: prevalence and associated risk factors . Journal of Neurosciences in Rural Practice 1 , 76–81. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC and Vandenbroucke JP (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies . Annals of Internal Medicine 147 , 573–577. [ PubMed ] [ Google Scholar ]
- Wakefield MA, Loken B and Hornik RC (2010) Use of mass media campaigns to change health behaviour . Lancet (London, England) 376 , 1261–1271. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- World Health Organization (2018) Global Status Report on Alcohol and Health-2018 . Geneva: WHO. [ Google Scholar ]
- IAS Preparation
- UPSC Preparation Strategy
What is the Prevalence of Drug Abuse in India?
In order to find the prevalence of drug abuse in India, a study was conducted by the Ministry of Social Justice and Empowerment (MoSJE). As per the 2019 report, 14.6% of the population uses alcohol. It is higher among men than women. It was found that 2.8% of the population uses Cannabis. This article covers the causes and harmful effects of drug abuse.
Aspirants would find this topic very helpful in the IAS Exam .
States with Highest Prevalence of Cannabis are
- Uttar Pradesh
- Chhattisgarh
India is sandwiched between the two largest Opium producing regions of the world that is the Golden triangle on one side and the Golden crescent on the other.
- The golden crescent area includes Pakistan, Afghanistan and Iran. Further details on the Golden Cresent are available on the linked page.
- The golden triangle area comprises Thailand, Myanmar, Vietnam and Laos, Read in detail about the Golden Triangle on the given link.
What are the Causes of Drug Abuse?
Some of the causes behind drug abuse are listed below.
- Family history of addiction
- Mental health disorder
- Peer pressure
- Lack of family involvement
- Taking highly addictive drugs.
What are the Different Types of Substance Abuse?
The 8 different types of substance abuse are listed below.
- Amphetamine Stimulants
- Hallucinogens
What are the Harmful Effects of Drug Abuse?
The harmful effects of drug abuse could be short-term or long-term. It could have a direct or indirect impact. The effects also depend on the type of drugs used. Short-term effects are listed below.
- Change in heart rate
- Change in blood pressure
- Heart attack
- Change in appetite
The long-term effects are listed below.
- Heart disease
- Lung disease
The magnitude of Substance Abuse in India – 2019 Report
As per Magnitude of Substance Abuse in India 2019 report
- 72 lakhs people need treatment for using Cannabis
- 11 lakhs people need treatment for using sedatives
- 60 lakhs people need treatment for using Opioids.
- It was estimated there are around 16 crore alcohol consumers in the 10-75 years age group in India.
- 5.7 crore people needed treatment for using alcohol.
Reasons for Drug Abuse
- To be accepted by the peers
- Increasing economic stress
- Changing cultural values
- Experimentation
- Neurotic pleasure
- Ineffective Policing
Drug Abuse – Negative Impacts
Some of the negative impacts of drug abuse are given below
- Increase in diseases like HIV, Hepatitis B and C, Tuberculosis
- Increase in violence
- Economic potential gets wasted
- Affects relationships with family, friends creating emotional and social problems
- Increases financial burden
- Women face domestic violence
India – Signatory of Various International Treaties and Conventions to Combat Drug Menace
United Nations General Assembly (UNGA) on 7th December 1987, decided that 26th June of every year will be recognized as the International Drug Day (another name for International Day against Drug Abuse & Illicit Trafficking). Further details on International Drug Day are available on the given link.
India is a signatory of the following international treaties and conventions to combat the menace of Drug Abuse
- United Nations (UN) Convention on Narcotic Drugs (1961)
- United Nations (UN) Convention on Psychotropic Substances (1971).
- United Nations (UN) Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances (1988)
- Transnational Convention Crime (2000)
Drug Abuse and WHO
WHO has played an important role within the UN system in addressing the world drug problem. WHO activities to counter the world drug problem can be presented under the following main dimensions:
- prevention of drug use and reduction of vulnerability and risks;
- treatment and care of people with drug use disorders;
- prevention and management of the harms associated with drug use;
- access to controlled medicines; and
- monitoring and evaluation.

Target 3.5 of UN Sustainable Development Goal 3 sets out a commitment by governments to strengthen the prevention and treatment of substance abuse. You can go through the details on Sustainable Development Goals SDGs on the linked page.
Battle Against Drug Abuse in India – Recent Developments
- Government will roll out its Action Plan for 2020-21 known as Nasha Mukt Bharat.
- The Focus of the plan will be to build treatment and drug de-addiction facilities in 272 districts identified as vulnerable based on access to drugs and prevalence of substance abuse.
- The Action plan will be steered by the Ministry of Social Justice and Empowerment. (MSJE).
- Among the 272 Vulnerable districts identified Uttar Pradesh has 33 vulnerable districts, Punjab (18 districts), Delhi (11 districts), Gujarat (8 districts) and Maharashtra (Pune, Mumbai, Nashik, Nagpur).
Nasha Mukt Bharat Action Plan 2020-21 – Ministry of Social Justice and Empowerment
The main components and 3 pronged strategies of Nasha Mukt Bharat are given below.
Nasha Mukt Bharat will focus on 3 pronged strategies, which are listed below.
- Treatment through the Health Departments.
- Outreach/Awareness by Social Justice
- Narcotics Bureau
Nasha Mukt Bharat – Main Components of the Action Plan 2020-21
- Awareness generation programs in University Campuses Higher Education institutions, and schools.
- Building capacity for service providers
- Focus on Treatment facilities in Hospital Settings.
- Identification of dependent population and community outreach.
The above details would help candidates prepare for UPSC 2023 .
Frequently Asked Questions about Drug Abuse in India
Which state consumes highest drugs in india, what are ethical issues in drug abuse.
Related Links
Leave a Comment Cancel reply
Your Mobile number and Email id will not be published. Required fields are marked *
Request OTP on Voice Call
Post My Comment
IAS 2024 - Your dream can come true!
Download the ultimate guide to upsc cse preparation.
- Share Share
Register with BYJU'S & Download Free PDFs
Register with byju's & watch live videos.
A Brand of CLT Technologies & Edu-Publishers Pvt. Ltd.
Forgot password
If you haven’t created your account yet, please SIGN UP HERE
Quick Links Testimonials FAQ
Hybrid Classes
We provide offline, online and recorded lectures in the same amount.
Personalised Mentoring
Every aspirant is unique and the mentoring is customised according to the strengths and weaknesses of the aspirant
Topicwise Mindmaps
In every Lecture. Director Sir will provide conceptual understanding with around 800 Mindmaps.
Quality Content
We provide you the best and Comprehensive content which comes directly or indirectly in UPSC Exam.
If you haven’t created your account yet, please SIGNUP HERE
UPSC Courses
IAS Foundation 2024
- C2U-NCERT 2024
- Newspaper Analysis Program
- Basic Daily Answer Writing
Optional Classes
- Geography Crash Course
Current Affairs
- Daily Newspaper Analysis - DNA
- UPSC Facts & Data
- GS Prelims PT Pointers
- Press Information Bureau - PIB
- Good Morning Times - Subject Wise
- EASY TO PICK MONTHLY CURRENT
- GS Paper Wise Current Affairs
- Daily Question Practice (PT-Mains)
Test Series
- RAW Live MCQ
- Oral Test Session By Director Sir
Others Links
- Testimonials
UPSC Prelims Classes 2024
Crash Course
- Sanjeevani @ 60Days
- Morden History
- Science & Technology
Regular Modules 2024
- Mapping & Geography
- Environment
- Economics Basic To Advance
- Polity & History
- News Paper Analysis Programme
- Prelims Test Series
- About Civil Services
- UPSC Prelims Syllabus & Strategy
- UPSC Previous Years Paper
- Prelims Modular Batches
- UPSC Prelims - PT Pointers
- Exclusive Test Series - Mock
- CSAT Classes
- Prelims Sanjeevani 2024 Crash Course
Mains Classes 2024
- RAW GS Crash Course
- Target 50 Program
- Ethics & Case Studies
- Editorial & Current Affairs – QIP
- Writing Skill Development Program
Mains & Interview
- Mains Syllabus & Strategy
- Daily UPSC Answer Writing
- Target 50 For Mains Batch
- Personality Test
- Mains Crash Course
- MAINS Previous Papers
- Optionals Previous Papers
Mains Material
- Mains Kunji
- Prelims (Live-MCQ)
- Prelims PT Tricks-2024
- Daily Answer Writing
Free Study Material
- Important Video Lectures
- Previous Years Papers
- Newspaper Analysis & ENY Notes
- UPSC GS Mains Notes
- 2 nd ARC Report Summary
- Aspire IAS Notes
- Free Download - UPSC Content
- Paid Material(SLP)
- UPSC Optional Notes

DAILY NEWS ANALYSIS
- Download PDF
- SHARE ARTICLE
23 August, 2021
Drug Abuse in India
- Social issues
- Ministry of Social Justice
Although the use of various psychoactive substances such as alcohol, cannabis and opioids has been observed in India for centuries, the current dimension of the extent and pattern of psychoactive substance use and the problems associated with their use are not well documented.
The National Drug Dependence Treatment Centre (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi was entrusted with the responsibility to lead the technical and scientific aspects of the National Survey on Extent and Pattern for Substance Use in India which was conducted in all the 36 states and UTs of the country, in collaboration with ten other medical institutes and a network of 15 NGOs.
- Substance abuse exists in all population groups but adult men bear the brunt of substance use disorders.
- Alcohol is the most common psychoactive substance used by Indians. About 14.6% of population (between 10 to 75 years) consume alcohol. States with the highest prevalence of alcohol use are Chhattisgarh, Tripura, Punjab, Arunachal Pradesh and Goa.
- After Alcohol, Cannabis and Opioids are the next commonly used substances in India. About 2.8% of the population (3.1 crore individuals) reports having used any cannabis product within the previous year.
- It has been estimated that there are about 8.5 lakh people who inject drugs.
- Of the total cases estimated by the report, more than half of them are contributed by states like Punjab, Assam, Delhi, Haryana, Manipur, Mizoram, Sikkim and Uttar Pradesh.
- About 60 lakh people are estimated to need help for their opioid use problems.
- More and more children are taking to alcohol consumption and the highest percentage of children who are addicted to alcohol are in Punjab followed by West Bengal and Uttar Pradesh.
- According to NCRB data, in 2019, 7719 out of the total 7860 suicide victims due to drug abuse/alcohol addiction were male.
- Even in the data relating to deaths due to road accidents, drugs & alcohol are one of the most causative factors.
Reasons for use of drugs in India
- India is at the location between Golden Crescent (Iran, Afghanistan and Pakistan) and Golden Triange (Burma, Thailand, Laos and Vietnam) which are the two largest opium producing regions of the World.
- Students and Youth consume drugs as a stress buster from their studies or work pressure. It is generally seen that an unemployed youth, out of frustration, ends up in taking drugs.
- Peer pressure and other psychological factors like the glamour attached to it and out of fun can cause teens to engage in risky behaviours, leading to substance abuse.
- People in the lower income group who cannot have an adequate amount of food, take drugs to sleep or relax.
- The cause behind drug menace is the drug cartels, crime syndicates and ultimately the ISI which is the biggest supplier of drugs.
- The African as well as the Southasian route being misused to bring drugs into the country.
Impact of Drug Abuse
- Drug abuse leads to physical, psychological, moral and intellectual decay. This means wastage of economic potential of young generation.
- Drug addiction causes immense human distress. Incidence of eve- teasing, group clashes, assault and impulsive murders increase with drug abuse.
- Drug use can lead to social and emotional problems and can affect relationships with family and friends.
- Problems with memory, attention and decision-making, which make daily living more difficult.
- Illegal production and distribution of drugs have spawned crime and violence worldwide.
- Increase in incidences of HIV, hepatitis B and C and tuberculosis due to addiction adds the reservoir of infection in the community burdening the health care system further.
- Women in India face greater problems from drug abuse. The consequences include domestic violence and infection with HIV, as well as the financial burden.
International Efforts to fight Drug abuse
- The first International Day against Drug Abuse and Illicit Trafficking was observed by the UN General Assembly on June 26, 1987. Since then, every year, this day marks the coherent and seamless global cooperation to achieve a drug-free society. So far, the UN has organized three international conventions in 1961, 1971 and 1988. The first one sought to eliminate the illicit production and non-medical use of opioids, cannabis and cocaine . The meeting held in 1971 extended the scope to the psychotropic medications or synthetic drugs (e.g., amphetamines, barbiturates and LSD). The third convention against illicit trafficking was targeted at the suppression of the illegal global market, and the restriction was also extended to the precursor chemicals .
- India is also signatory to the following International treaties and conventions:
- United Nations (UN) Convention on Narcotic Drugs (1961)
- UN Convention on Psychotropic Substances (1971).
- UN Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances (1988)
- UN Convention against Transnational Organized Crime (UNTOC) 2000
Efforts by India to reduce Drug abuse
As enshrined in its constitution ( Article 47 ) and being one of the signatories of the United Nation's International Conventions, India had the onus act to eliminate the use of illicit drugs, to develop measures to prevent drug use and to ensure availability of treatment for people with drug use disorders.
India has adopted the three-pronged strategies - supply, demand and harm reduction .
Drug De-addiction Programme (DDAP)
- Following the 1971's UN Convention on Psychotropic Substances, the Ministry of Health and Family Welfare, Government of India, established an Expert Committee to look into the issue of drug and alcohol use in India.
- The Committee's report was submitted in 1977, and after approval from the Planning Commission, Drug De-addiction Programme (DDAP) was rolled out in 1985-1986.
- The primary aim of the DDAP was drug demand reduction .
The Narcotic Drugs and Psychotropic Substances (NDPS) Act, 1985
- India is a signatory to the UN Single Convention on Narcotics Drugs 1961, the Convention on Psychotropic Substances, 1971 and the Convention on Illicit Traffic in Narcotic Drugs and Psychotropic Substances, 1988 which prescribe various forms of control aimed to achieve the dual objective of limiting the use of narcotic drugs and psychotropic substances for medical and scientific purposes as well as preventing the abuse of the same.
- The primary aim of the NDPS was 'to prevent and combat drug abuse and illicit trafficking', an apparent emphasis on the supply reduction.
- The administrative and legislative setup in the field of Narcotics has been put in place in the country in accordance with the spirit of the UN Conventions.
- The basic legislative instrument of the Government of India in this regard is the Narcotics Drugs and Psychotropic Substances (NDPS) Act, 1985.
- The Act provides stringent provisions for the control and regulation of operations relating to narcotic drugs and psychotropic substances.
- It also provides for forfeiture of property derived from, or used in, illicit traffic in narcotic drugs and psychotropic substances.
- It also provides for death penalty in some cases where a person is a repeat offender.
National Fund for Control of Drug Abuse
- The consultative committee (an advisory committee formed by the NDPS Act), which was constituted in 1988, formulated a national-level policy to control drug abuse.
- The committee created a fund, National Fund for Control of Drug Abuse and involved a couple of other major stakeholders - the Ministry of Health (and Family Welfare) and the Ministry of Welfare (currently Social Justice and Empowerment).
- The Ministry of Health was entrusted with the job of prevention and treatment of drug dependence, whereas the Ministry of Welfare was assigned with the responsibility of the rehabilitation and social integration of people with drug dependence.
- The Ministry of Health established seven treatment centres during the first phase (in 1988).
- The aims of these centres were treatment, drafting of educational material and training of medical and paramedical staff to generate the future workforce to deal with the problem of drug abuse.
Other Policy and Schemes
- Over the last three decades, there has been a substantial expansion of services in all dimensions.
- The Ministry of Social Justice and Empowerment published the draft policy of the drug demand reduction, the National Drug Demand Reduction Draft Policy in 2013 .
- To scale up the existing services, the Ministry has rolled out the 'Central Sector Scheme of Assistance for Prevention of Alcoholism and Substance Abuse and Social Defence Services .'
- The Ministry of Social Justice has also published its five-year plan, 'National Action Plan for Drug Demand Reduction' in 2018.
- The Mental Health Care Act (2017) has included alcohol and drug use disorders under its ambit . This measure is likely to increase the adherence to the human rights, to ensure non-discrimination, the respect to the right to autonomy and confidentiality, to increase the availability and access to the minimum standard of care and rehabilitation for people with substance use disorders.
Nasha Mukt Bharat campaign
- This campaign launched this year in 2020, is run for 272 Most Affected Districts’ by the Ministry of Social Justice and Empowerment with focus on institutional support, community outreach and awareness generation.
- It focuses on a three-pronged strategy combining-
- Efforts of Narcotics Bureau,
- Outreach/Awareness by Social Justice and
- Treatment through the Health Dept.
- These districts are identified based on inputs from Narcotics Control Bureau (NCB) and findings of Comprehensive National Survey done by Ministry.
- Nasha Mukt Bharat Abhiyaan in 272 districts is from 15th August 2020 to 31st March 2021.
- Abhiyaan Action Plan has the following components:-
- Awareness generation programmes in the community and Youth in particular
- Focus on Higher Educational institutions, University Campuses and Schools
- Community outreach and identification of dependent population
- Focus on Treatment facilities in Hospital settings
- Capacity Building Programmes for Service Providers.
National Action Plan for Drug Demand Reduction (NAPDDR) for 2018-2025
- The Ministry of Social Justice and Empowerment has formulated and is implementing a National Action Plan for Drug Demand Reduction (NAPDDR) for 2018-2025 .
- The Plan aims at reduction of adverse consequences of drug abuse through a multi-pronged strategy.
- The activities under the NAPDDR, inter-alia, include awareness generation programmes in schools/colleges/Universities, workshops/seminars/ with parents, community based peer led interactions intervention programmes for vulnerable adolescent and youth in the community, provisioning of treatment facilities and capacity building of service providers.
- The Ministry has also initiated focused intervention programmes in vulnerable districts across the country with an aim to increase community participation and public cooperation in the reduction of demand for dependence-producing substances and promote collective initiatives and self-help endeavour among individuals and groups vulnerable to addiction or found at risk.
Way Forward
- Considering the enormous challenge of substance use disorders in the country, there is an urgent need of policies and programmes which can bring relief to the large number of affected Indian citizens.
- Scientific evidence-based treatment needs to be made available for people with Substance use disorders.
- A coordinated, multi-stakeholder response will be necessary to scale-up treatment programmes in the country.
- Evidence-based substance use prevention programmes are needed to protect the young people.
- A conducive legal and policy environment is needed to help control drug problems.
- Harm reduction needs to be embraced widely as a philosophy to deal with substance use.
- Prevention of drug abuse and its health and psychosocial impact should be made part of the curriculum from the upper primary level.
- Revival of school clubs for early identification of drug users and expert intervention and setting up of suggestion box in schools.
- Awareness building and educating people about ill effects of drug abuse.
- Community based intervention for motivational counselling, identification, treatment and rehabilitation of drug addicts.
- Training of volunteer/service providers and other stakeholders with a view to build up a committed and skilled cadre.
- Undertake drug demand reduction efforts to address all forms of drug abuse including dependence related to the consumption of two or more substances at the same time.
- Drug menace is the manifestation of deep-rooted distortions in the socio-cultural, economic and political system. Being systemic and multi-dimensional, its solution shall have to be systemic and multi-pronged.
- It is emphasized the need of preventive, punitive and curative measures to tackle the menace.
- There is an urgent need to understand the complexity of the problem having far-reaching social, economic and political implications.
- There is a need to address all these factors responsible for drug menace in the region as punitive measures alone cannot uproot this menace.

Ministry of Minority Affairs-Year review
The Ministry was carved out of Ministry of Social Justice & Empowerment in 2006. Objective- To ensure a more focused approach towards issues relating to the notified minority communities - Muslim, Christian, Buddhist, Sikhs, Parsis and Jain. As per Census 2011, around 19.3% of the population belongs to minorities. Mandate- To f

Indian Railways in 2023 – Year Review
The Performance of Indian Railways in 2023 showed significant strides in infrastructure but reveals underwhelming freight loading and financial performance. How Indian Railways performed in 2023? Near completion of DFC – Dedicated Freight Corridors are nearing completion with more than 200 freight trains already runnin

Global Nuclear Order and Geopolitics
The Global Nuclear Order refers to the international system, agreements, norms, and structures that govern and regulate the use, possession, proliferation, and control of nuclear weapons and nuclear energy worldwide. It encompasses a complex network of treaties, agreements, and norms that have evolved over time to manage the risks associated wit
Supreme Court Judgments in 2023
The Supreme Court has delivered several landmark judgments in 2023. S.No Name of the Case Judgement 1 Vivek Narayan Sharma v. Union of India Upheld the decision taken by the Union Government to demonetise currency notes of Rs. 500 and Rs.10

Ministry of Health and Family Welfare – YEAR REVIEW
The Ministry is charged with health policy in India, which is also responsible for all government programs relating to family planning in India. Departments Department of Health and Family Welfare Department of Health Research Union Minister- Mansukh L. Mandaviya Health Missions National Health Mission (NHM) &
01 Feb,2024
Important gs topics.
- Union Budget 2024-25: Highlights –Interim Budget

Search By Date
Top editorials.
- Acculturation
- I2U2 FOOD PARK
- LABOUR CODE
- Organisation Of Turkic State and India-Turkey Relation
- MPLAD SCHEME
- Quantum Technology in India
- Non-Aligned Movement: Detailed Overview
- CLIMATE CHANGE AND COP 26
- Tribal Welfare
Saarthi Mentorship Programme
Our Popular Courses
Module wise Prelims Batches
Mains Batches
Important Tags
- Economic Issues
- International Relations
- Miscellaneous
- Human Geography
- Modern History
- Indian Society
- Art and Culture
- Government policies and interventions
- Biodiversity & Environment
- Bilateral Relations
- Important Bills
- Internal security
- Important reports
- Various acts
- International organisation
- International treaties and conventions
- Disaster and Disaster management
- Indian Polity
- World History
- Indian Geography
- Physical Geography
- Developmental Issues
- Indian Economy
- Government Policies & Reports
- Tolerance and Intolerance
- Ancient History
- Add To My Notes
Articles:Geography And Environment
Articles: history culture society, articles: governance & national issues, articles: ir & io, articles: economic development & economic issues, articles: s&t internal security, articles: ethics & others, articles: others, update my notes, newsletter subscription, important links.

Challenge UPSC 2024 - PT Tricks
Update Info
- Prelims Sanjeevani 2021 Crash Course
Mains & Interview
- Mains Sanjeevani 7Days Batch (coming soon)
- MAINS Test Series By Toppers
- RAW Prelims Live MCQ 2021
UPSC Resource
- General Studies Notes
- SLP - Paid Notes
Drug Abuse : A Social Evil | UPSC Mains Essay Preparation PDF Download
Drug Abuse : A Social Evil
(1) Opening — Social Awareness.
— Enslavement to drugs and compulsion to obtain and consume it by any means.
(2) Body — Different types of drugs.
— Explanation by psycholo-gists and sociologists.
— New dimension in drug abuge.
— Search for the causes of drug abuse.
— Drugs among children.
— Effects of drug.
— Laws are not so strict.
— Drug as a source of revenue.
(3) Closing — Drug abuse is a social problem and has legal ramification. War on drugs is on.
"Drug is Death : Say no to Drugs " and other such slogans visible on billboards and newspapers are proofs of the social awareness drug abuse has attracted. Drug related crimes are equally conscience stirring and have made people much over it.
We all have relied on the drugs. Our doctors have prescribed for the various diseases, so, how can its use be an abuse. The use of psychoactive substances for obtaining relief from mental tension or physical discomfort i.e. for therapeutic uses is legitimate use of drugs. Contrary to this, when used for attaining pleasure or new experiences and consequent physical or psychological harm is termed as drug abuse. Such drug abuse induces drug dependence and ultimately addiction and habituation. In drug addicts there is an enslavement to drugs and compulsion to obtain and consume it by any means. They develop a psychological and physical dependence on the effects of the drugs and an effect detrimental to the individual and to the society.
The abusable drugs are of various types; sedatives or depressants that relax the central nervous systems, induce sleep and provide a soothing effect. Stimulants activate the central nervous systems and relieve tensions, makes them aggressive and counteract fatigue. Narcotics, like depressants affect — the central nervous system and produce feelings of pleasure strength and lesson inhibitions. Hallucinogens produce distortion of perceptions and dream images.
Drug abuse has been explained by psychologists and sociologists. It is generally regarded that pleasurable sensations produced by drugs reinforce their use or it satisfies certain psychological needs, or is a response to fear and insecurity to the conditions of modern life, often association with users is also regarded as a reason for accepting drugs. Drug abuse can also be explained in terms of weakening of social bonds between individuals and society due to maladjustment alienation and non-commitments.
A new dimension in drug abuse has been its use by sports persons to enhance their potential beyond humanly endurable limits. The incident of Ben Johnson was a jolt to the sports lovers all over the world and has caused much thinking on effort to curb the recurrence of such incidents. However, with unfailing regularity such controversies erupt, for example Katrin Krabe.
It would be apropriate here to search for the causes of drug abuse. Among sports persons it can be safely attributed to the search and urge for glory. It can be an attempt to gain an unfair advantage over the others in the achievement orientation of modern society. The ends have become all powerful and means have been relegated as secondary.
The use of drugs among children which is most shocking and astoundign can be variously explained. Juvenile delinquents take to it in defiance and devisance to the social values. Some children accept it under peer group pressure and as an act of proving their 'masculinity. Others take to this due to weakening of emotional bonds between parents and siblings. The children who are in an impressionable age require much effectual and emotional bond to wean them away from such anti-social activities.
In rural areas the use of psychoactive substance is for religious purposes e.g. Holi, Shivratri and on ritual occasions. However, it is also used to relieve fatigue and also a source of entertainment.
In industrial urban setting the use is for more or less the same reasons.
Apart from the health and physical disadvantages drug abuse causes, it has also led to an acceleration in crime. An addict would stop at nothing to get his dose of the drug. There has been a spurt in thefts and murders by these addicts whose dependence physical and psychological upon the drugs is so great that the accepted values and norms of the society is shelved and their prime concern becomes acquiring their dosage.
There has been an increase in smuggling and peddling of those drugs as the economic advantages are numerous. It has also made the gangs engaged in such activities more vicious and violent as the economic stakes are very high.
This delineation of drug abuse brings us to the point where reference must be made to efforts to curb their evil. Given that the use of drugs have historical and cultural context makes prevention more complicated. Efforts have been made to combat drug trafficking, treat addicts and prevent drug abuse.
India being on the transit route faces a challenging and unenviable task. However, our Narcotics Drugs and Psychotropic Substances Act has not been very effective, Seizures have increased and so have indictment for offences but that is reflective only of the increase in those activities and not any positive development of control of drug abuse. Other legal sanctions are merely suggestions of intention and not actions.
Government regards drugs as a source of revenue and therefore its cultivation cannot be stopped. The inefficiency of administrative machinery in policing and preventing abuse needs no highlighting.
The only positive developments is the establishment of de-addiction and detoxification centers which have enabled us to salvage some people from destruction. However, these centres are expensive and the addicts have a tendency to relapse unless they have a strong will power and a desire to abdicate the malaise. Voluntary associations have also been doing a commendable task.
In conclusion, we can say that drug abuse has been realised as a major evil. It is a social problem and has legal ramifications. It has been given a high profile now and mass media has been disseminating information to educate people with the intention of preventing drug abuse. The battle continues and war on drugs is on.
Top Courses for UPSC
Faqs on drug abuse : a social evil - upsc mains essay preparation, how to prepare for upsc, objective type questions, drug abuse : a social evil | upsc mains essay preparation, sample paper, study material, video lectures, mock tests for examination, practice quizzes, extra questions, semester notes, past year papers, important questions, previous year questions with solutions, shortcuts and tricks, viva questions.
Drug Abuse : A Social Evil Free PDF Download
Importance of drug abuse : a social evil, drug abuse : a social evil notes, drug abuse : a social evil upsc questions, study drug abuse : a social evil on the app, welcome back, create your account for free.

Forgot Password
Unattempted tests, change country.
- Share full article
Advertisement
Supported by
A Conversation With …
Teen Drug Use Habits Are Changing, For the Good. With Caveats.
Dr. Nora Volkow, who leads the National Institutes of Drug Abuse, would like the public to know things are getting better. Mostly.

By Matt Richtel
Historically speaking, it’s not a bad time to be the liver of a teenager. Or the lungs.
Regular use of alcohol, tobacco and drugs among high school students has been on a long downward trend.
In 2023, 46 percent of seniors said that they’d had a drink in the year before being interviewed; that is a precipitous drop from 88 percent in 1979, when the behavior peaked, according to the annual Monitoring the Future survey, a closely watched national poll of youth substance use. A similar downward trend was observed among eighth and 10th graders, and for those three age groups when it came to cigarette smoking. In 2023, just 15 percent of seniors said that they had smoked a cigarette in their life, down from a peak of 76 percent in 1977 .
Illicit drug use among teens has remained low and fairly steady for the past three decades, with some notable declines during the Covid-19 pandemic.
In 2023, 29 percent of high school seniors reported using marijuana in the previous year — down from 37 percent in 2017, and from a peak of 51 percent in 1979.
There are some sobering caveats to the good news. One is that teen overdose deaths have sharply risen, with fentanyl-involved deaths among adolescents doubling from 2019 to 2020 and remaining at that level in the subsequent years.
Dr. Nora Volkow has devoted her career to studying use of drugs and alcohol. She has been the director of the National Institute on Drug Abuse since 2003. She sat down with The New York Times to discuss changing patterns and the reasons behind shifting drug-use trends.
What’s the big picture on teens and drug use?
People don’t really realize that among young people, particularly teenagers, the rate of drug use is at the lowest risk that we have seen in decades. And that’s worth saying, too, for legal alcohol and tobacco.
What do you credit for the change?
One major factor is education and prevention campaigns. Certainly, the prevention campaign for cigarette smoking has been one of the most effective we’ve ever seen.
Some of the policies that were implemented also significantly helped, not just making the legal age for alcohol and tobacco 21 years, but enforcing those laws. Then you stop the progression from drugs that are more accessible, like tobacco and alcohol, to the illicit ones. And teenagers don’t get exposed to advertisements of legal drugs like they did in the past. All of these policies and interventions have had a downstream impact on the use of illicit drugs.
Does social media use among teens play a role?
Absolutely. Social media has shifted the opportunity of being in the physical space with other teenagers. That reduces the likelihood that they will take drugs. And this became dramatically evident when they closed schools because of Covid-19. You saw a big jump downward in the prevalence of use of many substances during the pandemic. That might be because teenagers could not be with one another.
The issue that’s interesting is that despite the fact schools are back, the prevalence of substance use has not gone up to the prepandemic period. It has remained stable or continued to go down. It was a big jump downward, a shift, and some drug use trends continue to slowly go down.
Is there any thought that the stimulation that comes from using a digital device may satisfy some of the same neurochemical experiences of drugs, or provide some of the escapism?
Yes, that’s possible. There has been a shift in the types of reinforcers available to teenagers. It’s not just social media, it’s video gaming, for example. Video gaming can be very reinforcing, and you can produce patterns of compulsive use. So, you are shifting one reinforcer, one way of escaping, with another one. That may be another factor.
Is it too simplistic to see the decline in drug use as a good news story?
If you look at it in an objective way, yes, it’s very good news. Why? Because we know that the earlier you are using these drugs, the greater the risk of becoming addicted to them. It lowers the risk these drugs will interfere with your mental health, your general health, your ability to complete an education and your future job opportunities. That is absolutely good news.
But we don’t want to become complacent.
The supply of drugs is more dangerous, leading to an increase in overdose deaths. We’re not exaggerating. I mean, taking one of these drugs can kill you.
What about vaping? It has been falling, but use is still considerably higher than for cigarettes: In 2021, about a quarter of high school seniors said that they had vaped nicotine in the preceding year . Why would teens resist cigarettes and flock to vaping?
Most of the toxicity associated with tobacco has been ascribed to the burning of the leaf. The burning of that tobacco was responsible for cancer and for most of the other adverse effects, even though nicotine is the addictive element.
What we’ve come to understand is that nicotine vaping has harms of its own, but this has not been as well understood as was the case with tobacco. The other aspect that made vaping so appealing to teenagers was that it was associated with all sorts of flavors — candy flavors. It was not until the F.D.A. made those flavors illegal that vaping became less accessible.
My argument would be there’s no reason we should be exposing teenagers to nicotine. Because nicotine is very, very addictive.
Anything else you want to add?
We also have all of this interest in cannabis and psychedelic drugs. And there’s a lot of interest in the idea that psychedelic drugs may have therapeutic benefits. To prevent these new trends in drug use among teens requires different strategies than those we’ve used for alcohol or nicotine.
For example, we can say that if you take drugs like alcohol or nicotine, that can lead to addiction. That’s supported by extensive research. But warning about addiction for drugs like cannabis and psychedelics may not be as effective.
While cannabis can also be addictive, it’s perhaps less so than nicotine or alcohol, and more research is needed in this area, especially on newer, higher-potency products. Psychedelics don’t usually lead to addiction, but they can produce adverse mental experiences that can put you at risk of psychosis.
Matt Richtel is a health and science reporter for The Times, based in Boulder, Colo. More about Matt Richtel
COMMENTS
Why in News. Recently, people in a few villages of Jodhpur district's Bilara block, Rajasthan have come together to tackle Drug Addiction among the youth.. Key Points. Steps Taken By the Villagers: Boycott of persons consuming liquor, tobacco and narcotics.; Imposition of a penalty on the sellers and buyers of these substances.; Drug Addiction: It refers to the condition of being addicted to ...
An additional 5% of the population consume alcohol in a harmful way. The report highlighted that 1 in 5 alcohol users are affected by alcohol dependence and hence require urgent treatment. 11% of Indians are binge drinkers according to WHO. This is against a global average of 16%.
16 crore people (14.6%) between the age of 10 and 75 years are current users of alcohol, and out of them, 5.2% are alcohol dependents. About 3.1 crore individuals (2.8%) are cannabis users, and 72 lakh (0.66%) people suffer from cannabis problems. Overall opioid users 2.06% and nearly 0.55% (60 lakh) require treatment services/health
Increases financial burden due to diversion of funding and resources to other areas such as police patrolling and rehabilitation centres. Drug abuse seriously affects our health, security, peace and development. Drug dependence, low self esteem, hopelessness can lead to criminal action and even suicidal tendencies.
2. Critically examine the economics of Alcohol addiction in the countr (250 words) Reference: Indian Express Introduction: Alcohol is the most abused substance in India, according to the findings of a report "Magnitude of Substance Use in India", submitted by AIIMS in Feb 2019 to Ministry of Social Justice and Empowerment.There are believed to be 62.5 million people in India who at least ...
Growing Drugs and alcohol consumption in India is becoming a major health hazard and a social menace. State like Punjab, North - Eastern States, Jammu & Kashmir have become home of drug abuse. Hooch Tragedy: In recent incident, over 40 people died in Gujarat's Botad district; 7 years since Bihar liquor ban: 199 deaths, 30 hooch cases ...
Alcoholism - UPSC GS2. Alcohol is a subject in the State list under the seventh schedule of the Indian Constitution. Article 47 of the Directive Principle in the Constitution of India states that "The state shall undertake rules to bring about prohibition of the consumption except for medicinal purposes of intoxicating drinks and of drugs ...
UPSC Essentials: Case Study of the week- Fight for a drug-free community Every youth who destroys his life by drug addiction is a loss to our society. The solution-oriented case study discusses the issue of drug abuse and de-addiction programme that aspirants will find useful in GS I, essay and ethics.
The scheme seeks to benefit victims of alcohol and substance abuse. Under the scheme, non-governmental organisations have been entrusted with the responsibility for delivery of services and the Ministry bears substantial financial responsibility (90% of the prescribed grant amount). ... UPSC Prelims and Mains Exam - 13th April 2024; UPSC Quiz ...
The Congress party has termed prohibition a "total failure" and has pleaded for it to be revoked. The excise department had earned around ₹600 lakh (equivalent to ₹47 crore or US$6.6 million in 2019) prior to prohibition. It earned about ₹10 lakh (US$14,000) annually in NLTP Act related fines as of June 2014.
Fifty-five peer-reviewed papers and one report were eligible for inclusion in this review. Prevalence of ever or lifetime alcohol consumption ranged from 3.9% to 69.8%; and prevalence of alcohol consumption at least once in the past year ranged from 10.6% to 32.9%. The mean age for initiation of drinking ranged from 14.4 to 18.3 years.
Sales of alcohol have seen a growth rate of 8% in the past 3 years. Officially, Indians are still among the world's lowest consumers of alcohol—government statistics show only 21% of adult men and around 2% of women drink. But up to a fifth of this group—about 14 million people—are dependent drinkers requiring "help".
Fifty-five peer-reviewed papers and one report were eligible for inclusion in this review. Prevalence of ever or lifetime alcohol consumption ranged from 3.9% to 69.8%; and prevalence of alcohol consumption at least once in the past year ranged from 10.6% to 32.9%. ... parental use of alcohol or tobacco, non-contact sexual abuse and ...
Signs of Addiction to Drugs And Alcohol. Addictions and abuse of drugs and alcohol by teens are very common and can have serious consequences. In the 15-24-year age range, 50% of deaths (from accidents, homicides, suicides) involve alcohol or drug abuse. Drugs and alcohol also contribute to physical and sexual aggression, such as assault or rape.
Nasha Mukt Bharat Campaign: Nasha Mukt Bharat Abhiyaan (NMBA) was launched in 2020 to tackle the issue of Substance Abuse and a vision to make India Drug Free. It is a three-pronged attack combining: ... Certain crop drugs which have more than 50% alcohol and opioids need to be contained. ... UPSC Civil Services Examination, Previous Year ...
vegetarianism and abstinence from alcohol (Benegal, 2005). Meanwhile, during the British colonial rule, manufacturing of alcohol became restricted to licensed government distilleries, leading to the replacement of traditional alcoholic beverages to mass produced factory made products with greater alcohol content (Benegal, 2005).
A literature search was undertaken to review available published research papers, unpublished reports and anecdotal media information in the period 2000-2020 to assess the burden and pattern of alcohol use and appraise alcohol control policies in India. ... Alcohol use and its public health impact would continue to increase in India in the ...
Drug Abuse in India - Know about the different types of Substance Abuse, Major Causes, Harmful Effects, need for awareness, and Provisions Against the Drug Abuse. ... UPSC Previous Year Papers. UPSC 2023 Question Papers; UPSC 2022 Question Papers; UPSC 2021 Question Papers ... (Ministry of Social Justice and Empowerment) was surveyed to ...
Here are certain measures which need to be taken to prevent and control alcohol and drug abuse. Persistent counselling is required to teach the child to deal with failures, pressures, stress, and disappointments. In fact, guiding them towards productive activities such as music, painting, yoga, sports or one of their hobbies could also help.
As per the 2019 report, 14.6% of the population uses alcohol. It is higher among men than women. It was found that 2.8% of the population uses Cannabis. This article covers the causes and harmful effects of drug abuse. Aspirants would find this topic very helpful in the IAS Exam. Aspirants should begin their preparation by solving UPSC Previous ...
According to NCRB data, in 2019, 7719 out of the total 7860 suicide victims due to drug abuse/alcohol addiction were male. Even in the data relating to deaths due to road accidents, drugs & alcohol are one of the most causative factors. Reasons for use of drugs in India. India is at the location between Golden Crescent (Iran, Afghanistan and ...
Why in News. Recently, the Social Justice and Empowerment Ministry has recommended that the National Fund to Control Drug Abuse should be used to carry out de-addiction programmes, rather than just policing activities.. A proposal to decriminalise possession of small quantities of drugs, as defined in the Narcotic Drugs and Psychotropic Substances (NDPS) Act, 1985, had also been sent to the ...
Download the App. Drug Abuse : A Social Evil. structure. (1) Opening — Social Awareness. — Enslavement to drugs and compulsion to obtain and consume it by any means. (2) Body — Different types of drugs. — Explanation by psycholo-gists and sociologists. — New dimension in drug abuge. — Search for the causes of drug abuse.
A systemic review conducted by Nadkarni et al. [1] observed that the prevalence of ever or lifetime alcohol consumption in adolescence age between 10 and 24 years in India ranged from 3.9% to 69.8 ...
Illicit drug use among teens has remained low and fairly steady for the past three decades, with some notable declines during the Covid-19 pandemic. In 2023, 29 percent of high school seniors ...