- Share full article
Advertisement
Supported by
A Conversation With …

Teen Drug Use Habits Are Changing, For the Good. With Caveats.
Dr. Nora Volkow, who leads the National Institutes of Drug Abuse, would like the public to know things are getting better. Mostly.

By Matt Richtel
Historically speaking, it’s not a bad time to be the liver of a teenager. Or the lungs.
Regular use of alcohol, tobacco and drugs among high school students has been on a long downward trend.
In 2023, 46 percent of seniors said that they’d had a drink in the year before being interviewed; that is a precipitous drop from 88 percent in 1979, when the behavior peaked, according to the annual Monitoring the Future survey, a closely watched national poll of youth substance use. A similar downward trend was observed among eighth and 10th graders, and for those three age groups when it came to cigarette smoking. In 2023, just 15 percent of seniors said that they had smoked a cigarette in their life, down from a peak of 76 percent in 1977 .
Illicit drug use among teens has remained low and fairly steady for the past three decades, with some notable declines during the Covid-19 pandemic.
In 2023, 29 percent of high school seniors reported using marijuana in the previous year — down from 37 percent in 2017, and from a peak of 51 percent in 1979.
There are some sobering caveats to the good news. One is that teen overdose deaths have sharply risen, with fentanyl-involved deaths among adolescents doubling from 2019 to 2020 and remaining at that level in the subsequent years.
Dr. Nora Volkow has devoted her career to studying use of drugs and alcohol. She has been the director of the National Institute on Drug Abuse since 2003. She sat down with The New York Times to discuss changing patterns and the reasons behind shifting drug-use trends.
What’s the big picture on teens and drug use?
People don’t really realize that among young people, particularly teenagers, the rate of drug use is at the lowest risk that we have seen in decades. And that’s worth saying, too, for legal alcohol and tobacco.
What do you credit for the change?
One major factor is education and prevention campaigns. Certainly, the prevention campaign for cigarette smoking has been one of the most effective we’ve ever seen.
Some of the policies that were implemented also significantly helped, not just making the legal age for alcohol and tobacco 21 years, but enforcing those laws. Then you stop the progression from drugs that are more accessible, like tobacco and alcohol, to the illicit ones. And teenagers don’t get exposed to advertisements of legal drugs like they did in the past. All of these policies and interventions have had a downstream impact on the use of illicit drugs.
Does social media use among teens play a role?
Absolutely. Social media has shifted the opportunity of being in the physical space with other teenagers. That reduces the likelihood that they will take drugs. And this became dramatically evident when they closed schools because of Covid-19. You saw a big jump downward in the prevalence of use of many substances during the pandemic. That might be because teenagers could not be with one another.
The issue that’s interesting is that despite the fact schools are back, the prevalence of substance use has not gone up to the prepandemic period. It has remained stable or continued to go down. It was a big jump downward, a shift, and some drug use trends continue to slowly go down.
Is there any thought that the stimulation that comes from using a digital device may satisfy some of the same neurochemical experiences of drugs, or provide some of the escapism?
Yes, that’s possible. There has been a shift in the types of reinforcers available to teenagers. It’s not just social media, it’s video gaming, for example. Video gaming can be very reinforcing, and you can produce patterns of compulsive use. So, you are shifting one reinforcer, one way of escaping, with another one. That may be another factor.
Is it too simplistic to see the decline in drug use as a good news story?
If you look at it in an objective way, yes, it’s very good news. Why? Because we know that the earlier you are using these drugs, the greater the risk of becoming addicted to them. It lowers the risk these drugs will interfere with your mental health, your general health, your ability to complete an education and your future job opportunities. That is absolutely good news.
But we don’t want to become complacent.
The supply of drugs is more dangerous, leading to an increase in overdose deaths. We’re not exaggerating. I mean, taking one of these drugs can kill you.
What about vaping? It has been falling, but use is still considerably higher than for cigarettes: In 2021, about a quarter of high school seniors said that they had vaped nicotine in the preceding year . Why would teens resist cigarettes and flock to vaping?
Most of the toxicity associated with tobacco has been ascribed to the burning of the leaf. The burning of that tobacco was responsible for cancer and for most of the other adverse effects, even though nicotine is the addictive element.
What we’ve come to understand is that nicotine vaping has harms of its own, but this has not been as well understood as was the case with tobacco. The other aspect that made vaping so appealing to teenagers was that it was associated with all sorts of flavors — candy flavors. It was not until the F.D.A. made those flavors illegal that vaping became less accessible.
My argument would be there’s no reason we should be exposing teenagers to nicotine. Because nicotine is very, very addictive.
Anything else you want to add?
We also have all of this interest in cannabis and psychedelic drugs. And there’s a lot of interest in the idea that psychedelic drugs may have therapeutic benefits. To prevent these new trends in drug use among teens requires different strategies than those we’ve used for alcohol or nicotine.
For example, we can say that if you take drugs like alcohol or nicotine, that can lead to addiction. That’s supported by extensive research. But warning about addiction for drugs like cannabis and psychedelics may not be as effective.
While cannabis can also be addictive, it’s perhaps less so than nicotine or alcohol, and more research is needed in this area, especially on newer, higher-potency products. Psychedelics don’t usually lead to addiction, but they can produce adverse mental experiences that can put you at risk of psychosis.
Matt Richtel is a health and science reporter for The Times, based in Boulder, Colo. More about Matt Richtel
This website uses cookies.
By clicking the "Accept" button or continuing to browse our site, you agree to first-party and session-only cookies being stored on your device to enhance site navigation and analyze site performance and traffic. For more information on our use of cookies, please see our Privacy Policy .
- Journal of Economic Perspectives
- Summer 2008
Peer Effects and Alcohol Use among College Students
- Michael Kremer
- Article Information
- Comments ( 0 )
JEL Classification
- J13 Fertility; Family Planning; Child Care; Children; Youth
Mobile Menu Overlay
The White House 1600 Pennsylvania Ave NW Washington, DC 20500
The Economics of Administration Action on Student Debt
Higher education financing allows many Americans from lower- and middle-income backgrounds to invest in education. However, over the past 30 years, college tuition prices have increased faster than median incomes, leaving many Americans with large amounts of student debt that they struggle or are unable to, pay off.
Recognizing the burden of this debt, the Biden-Harris Administration has pursued two key strategies for debt reduction and cancellation. The first, student debt relief (SDR), aims to address the ill effects of flaws in the student debt system for borrowers. The second, the SAVE plan, reforms the federal student loan system, improving student loan affordability for future students and providing current graduates with breathing room during the beginning of a new career.
This issue brief examines the factors that precipitated the current student debt landscape, and details how both SDR and SAVE will enhance the economic status of millions of Americans with student debt: enabling them to allocate more funds towards basic necessities, take career risks, start businesses, and purchase homes. This brief highlights credible research, underscoring how the Administration’s student debt relief could boost consumption in the short-term by billions of dollars and could have important impacts on borrower mental health, financial security, and outcomes such as homeownership and entrepreneurship. This brief also details how the SAVE plan makes repaying college costs more affordable for current borrowers and future generations. CEA simulations show that, under SAVE, an average borrower with a bachelor’s degree could save $20,000 in loan payments, while a borrower with an associate degree could see nearly 90 percent savings compared to the standard loan repayment plan. These changes enable more people to pursue education and contribute to the broader economy.
Why do borrowers need relief?
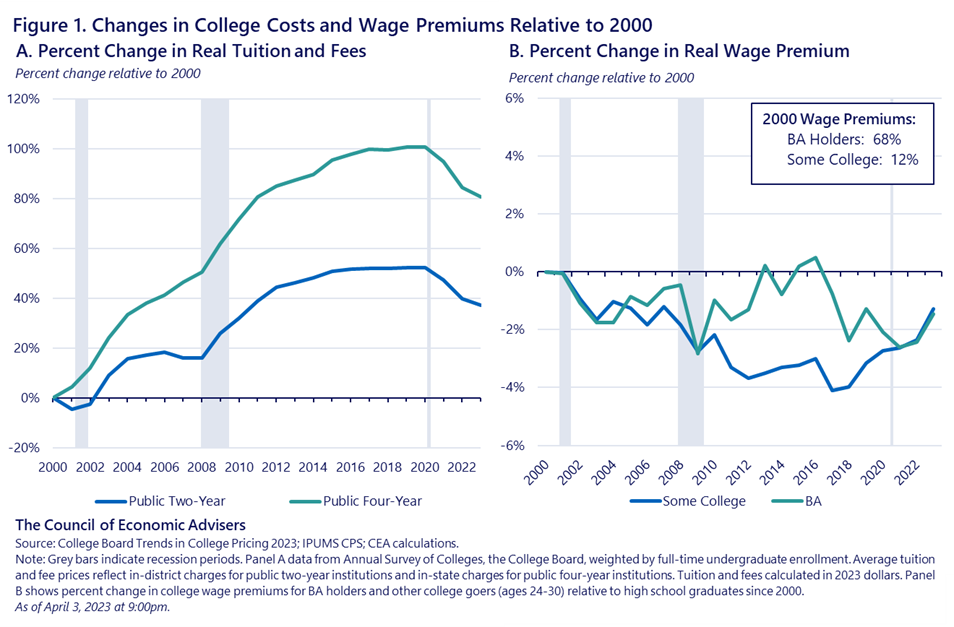
Over the last 20 years especially, the sticker price of college has risen significantly. Despite recent minor declines, sticker prices at public universities (which over 70% of undergraduate students in the United States attend) are 56% higher today than two decades ago. [1] While there are many reasons for this trend, the most rapid increases in tuition often occur during economic downturns as tuitions grow to fill the budgetary holes that are left when states cut their support to public colleges ( Webber, 2017 ; Deming and Walters 2018 ). This is especially problematic given many people choose to return to school during economic downturns ( Betts and MacFarland 1995 ; Hillman and Orians 2013 ). Unfortunately, contracting state appropriations have played a role in shifting the responsibility of financing away from public subsidies and toward students and families ( Turner and Barr, 2013 ; Bound et al., 2019 )–leading many students to take on more debt.
At the same time that college sticker prices have risen, the wage premium (the earnings difference between college goers and high school graduates) has not seen analogous growth. While obtaining a college degree remains a reliable entry point to the middle class, the relative earning gains for degree holders began to stagnate in the early 2000s after increasing for several decades. As shown in Figure 1b, since 2000, the wage premium for both bachelor’s degree holders and those with “some college” education (which includes anyone who enrolled in college but didn’t earn a BA) saw declines around the 2001-02 and 2008-10 recessions and a slow, inconsistent recovery thereafter. The decline is particularly notable for students who didn’t complete a four-year degree, a group that includes two-year college enrollees who have among the highest student loan default rates. [2]
Traditional economic theory tells us that individuals choose to invest in post-secondary education based on the expected costs and wage returns associated with the investment. But rapid and unforeseeable rises in prices and declines in college wage premia have contributed to decades of “unlucky” college-entry cohorts affected by a form of recessionary scarring . For example, a student who entered college in 2006 would have expected a sticker price of roughly $8,800 per year for a four-year college, but actually faced tuition of over $10,000 in their final year of college, a roughly 15% difference. This same student, upon graduation if they worked full time, would have earned about $3,500 less, on average, than what they would have expected upon entering. This example illustrates that many borrowers made sound borrowing decisions with available information, but as a result of these trends ended up with more debt than they could afford to pay off. [3] Consistent with this notion, the default rate for “unlucky” college entry cohorts of the 2000s is much higher than those of other cohorts, with undergraduate default rates doubling between 2000 and 2010: in 2017, 21 percent of undergraduate loan holders and 6 percent of graduate loan holders defaulted within 3 years ( CBO, 2020 ).
It is important to note that sticker prices for public institutions have declined 7 percent since 2021, the same period over which college wage premiums have been rising. Declining tuition, for the first time in decades, coincided with increased investment in higher education through pandemic-era legislation such as the American Rescue Plan, which allocated $40 billion in 2021 to support institutes of higher education and their students. Despite these improvements, as well as significant advances in the return on college investments over the last three years, many current borrowers still need some relief. The Administration has taken significant action to protect future cohorts from similar risks.
How the Administration is providing relief
Retrospective: Student Debt Relief Helps Existing Borrowers
In a commitment to help those who are overburdened with debt, the Administration has already approved Federal student debt cancellation for nearly 4 million Americans through various actions. Today , the Administration announced details of proposed rules that, if finalized as proposed, would provide relief to over 30 million borrowers when taken together with actions to date.
Importantly, much of this debt forgiveness comes from correcting program administration and improving regulations related to laws that were on the books before this Administration took office. This debt relief has affected borrowers from all walks of life, including nearly 900,000 Americans who have dedicated their lives to public service (such as teachers, social workers, nurses, firefighters, police officers, and others), borrowers who were misled and cheated by their institutions, and borrowers who are facing total or permanent disability, including many veterans. By relieving these borrowers of long-held, and in some cases very large burdens of debt, relief can have significant meaning and impact for borrowers, families, and their communities.
By reducing debtors’ liabilities, debt relief raises net worth (assets, including income less liabilities). Debt relief can also ease the financial burden of making payments—leading to greater disposable income for borrowers and their families, which enhances living standards and could positively influence decisions about employment, home buying, and mobility. While there are few direct estimates of the effect of debt cancelation in the literature, estimates based on the relationship between wealth and consumption suggest that this forgiveness could increase consumption by several billions of dollars each year in the next five to ten years.
Additionally, a recent study suggests that student debt cancellation can lead to increased earnings (due to greater geographic and career mobility), improved credit scores, and lower delinquency rates on other debts ( Di Maggio, Kalda, and Yao, 2019 ). This can facilitate access to capital for starting a business or buying a car or home. As home mortgages often require a certain debt-to-income ratio and depend heavily on credit scores, student debt cancellation could potentially increase home ownership. Indeed, based on the mechanical relationship between housing industry affordability standards and debt-to-income ratios, industry sources have suggested that those without student debt could afford to take out substantially larger mortgages ( Zillow, 2018 ). Other research also indicates a negative correlation between student loan debt and homeownership ( Mezza et al., 2020 ).
It is important to note that, while these pecuniary benefits are important, the benefits associated with debt relief are not merely financial. Experimental evidence has linked holding debt to heightened levels of stress and anxiety ( Drentea and Reynolds, 2012 ), worse self-reported physical health ( Sweet et al., 2013 ), and reduced cognitive capacity ( Robb et al., 2012 ; Ong et al., 2019 ). Studies also show that holding student debt can be a barrier to positive life cycle outcomes such as entrepreneurship ( Krishnan and Wang, 2019 ), and marriage ( Gicheva, 2016 ; Sieg and Wang, 2018 ). Student debt relief has the potential to improve these key outcomes for millions of borrowers.
Prospective: The SAVE Plan Helps Prevent Future Challenges
To address unaffordable education financing moving forward, the Administration has also introduced the Saving on a Valuable Education (SAVE) loan repayment program. The SAVE plan prospectively helps student borrowers by ensuring that once they graduate, they never have to pay more than they can afford towards their student loan debt. Importantly, the SAVE plan protects borrowers from being “unlucky” by ensuring that high tuition or low earnings do not result in loan payments that borrowers can’t afford. The CEA has detailed the real benefits of SAVE for borrowers in issue briefs and blogs , underscoring that SAVE is the most affordable student loan repayment program in U.S. history. By substantially reducing monthly payment amounts compared to previous income driven repayment (IDR) plans and reducing time to forgiveness to as little as 10 years for people who borrowed smaller amounts, the SAVE plan can mean tens of thousands of dollars in real savings for borrowers over the course of repayment.
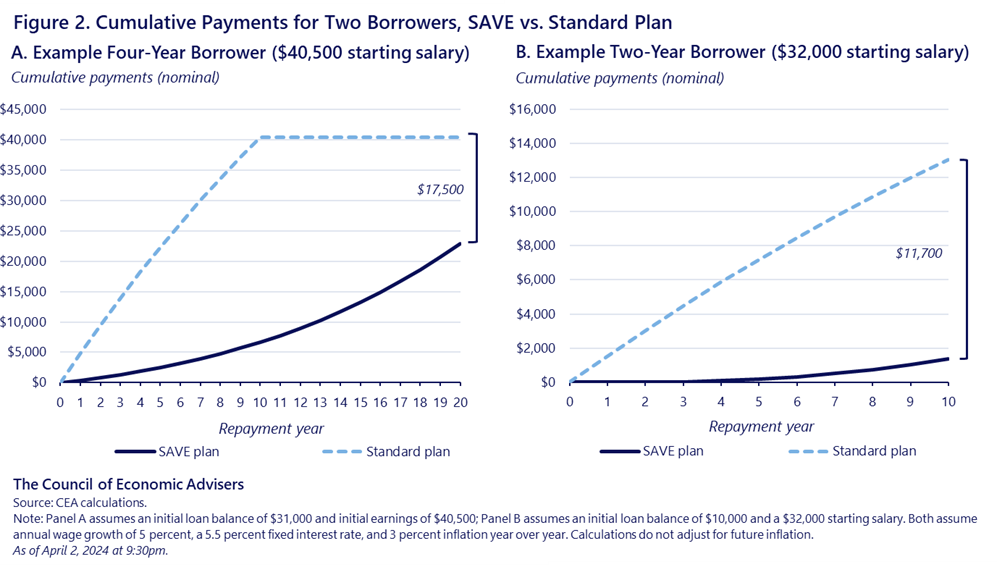
Figure 2 gives the example of two representative borrowers. Take the first, a 4-year college graduate who has $31,000 in debt and earns about $40,500 per year. Under a standard repayment plan, this borrower would pay roughly $330 dollars each month for 10 years. Under SAVE, this borrower would pay about $50 per month for the first ten years, and on average about $130 per month for the next 10 years. Over a 20-year period, this borrower would make roughly $17,500 less in payments, not accounting for inflation over that period. This represents a 56 percent reduction in total payments compared to the standard repayment plan and includes considerable loan forgiveness. Similarly, the representative 2-year college graduate has $10,000 in debt and earns about $32,000 per year. Under a standard plan, this borrower would pay $110 dollars each month for 10 years. Under SAVE, this borrower would pay $0 per month for the first two years, and under $20 per month for the next eight years before their debt is forgiven at year 10. Overall, this borrower would be responsible for roughly $11,700 less in lifetime payments, not accounting for inflation. This borrower sees nearly 90 percent savings compared to the standard plan and receives considerable loan forgiveness.
SAVE can also have benefits beyond the individual borrower. More money in borrowers’ pockets due to lower payment obligations under SAVE could boost consumption and give borrowers breathing room to make payments on other debt. This consumption effect is bolstered by a large literature documenting the benefits of easing liquidity constraints (see, for example, Aydin, 2022 ; Parker et al., 2022 ). Additionally, by shortening time to forgiveness for undergraduate borrowers, SAVE can lead to positive debt-relief outcomes (as discussed above) for many more borrowers.
Another key aspect of income-driven repayment plans like SAVE is that they protect borrowers from having to make large payments when incomes are low. Specifically, the required payments are not based on the initial loan balance, but on one’s income and household size so that those cohorts who need to borrow more to pay for college do not make larger payments unless they make more income. SAVE also protects more of a borrower’s income as discretionary and, when the full plan is implemented in Summer 2024, will limit monthly payments on undergraduate loans to 5 percent of discretionary income. In fact, for single borrowers who make less than $33,000 per year, the required monthly payments will be zero dollars. From a finance perspective, the SAVE plan provides a form of insurance against tuition spikes and economic downturns–taking some of the risk out of investing in one’s education while also bringing costs down.
A common concern, and one that could mute these benefits, is that increases in the generosity of education financing may encourage institutions to raise tuition and fees in response, a phenomenon commonly referred to as the Bennett Hypothesis (for an excellent overview of research, see Dynarski et al., 2022 ). Theoretically, in a market when sellers are maximizing profits, any policy that increases demand will also increase prices. However, this is less likely to impact the over 70% of U.S. undergraduates who attend public colleges, which are not profit-driven and often have statutorily set tuition. Consistent with this notion, the evidence in support of the Bennett Hypothesis primarily comes from for-profit colleges, which are highly reliant on students who receive federal financial aid ( Cellini and Goldin, 2014 ; Baird et al, 2022 ). [4] Importantly, although the for-profit sector enrolls some of the country’s most vulnerable students, enrollment in the sector in 2021 accounted for only 5 percent of total undergraduate enrollment, suggesting that aggregate tuition increases in response to changes in education financing may be modest. Furthermore, the Biden-Harris Administration has taken action to crack down on for-profit colleges that take advantage of, or mislead, their students. And, recent regulations, such as the Gainful Employment ( GE ) rule, add safeguards against unaffordable debt regardless of more generous education financing.
Although the SAVE plan stands to benefit borrowers of all backgrounds, the plan has important racial and socioeconomic equity implications because it is particularly beneficial for those borrowers with the lowest incomes. Centuries of inequities have led to Black, Hispanic, and Native households being more likely than their White peers to fall in the low end of the income distribution. This means that, mechanically, the SAVE plan’s benefits could accrue disproportionately to these groups. Indeed, using completion data from recent years, an Urban Institute analysis estimates that 59 percent of credentials earned by Black students and 53 percent of credentials earned by Hispanic students are likely to be eligible for some amount of loan forgiveness under SAVE, compared to 42 percent of credentials earned by White students ( Delisle and Cohn, 2023 ). Finally, the interest subsidy described in an August 2023 CEA blog , prevents ballooning balances when a borrower cannot cover their entire monthly interest payment, a phenomenon that has historically led to many borrowers in general, and Black borrowers in particular, to see loan balances that are higher than their original loan amount, even several years out from graduating with a bachelor’s degree ( NCES, 2023 ).
Broader economic impacts
The benefits associated with SDR and SAVE for millions of Americans are considerable. In the short run, under both SDR and SAVE, those who receive relief may be able to spend more in their communities and contribute to their local economies. Summing the likely consumption effects of the Administration’s student debt relief and SAVE programs results in billions of dollars in additional consumption annually. Despite the modest effect on the macroeconomy as a whole (note that the U.S. economy is roughly $28 trillion with a population of roughly 320 million), these consumption effects represent incredibly meaningful impacts on individual borrowers’ financial security and the economic wellbeing of their communities.
SAVE, because it brings down the cost of taking out loans to go to college, has the potential to lead to longer-term economic growth if it leads to greater educational attainment. This increased attainment can occur both through improved retention and completion of post-secondary education, and also the movement of students into college who would not have otherwise enrolled. There is a long macroeconomics literature linking educational attainment in a nation to GDP growth (see, for example, Lucas, 1988 ; Hanushek and Woesmann, 2008 ). While identifying the causal effect of schooling on GDP is challenging, researchers, using a variety of approaches, find that a one-year increase in average education (for the entire working population) would increase the real GDP level by between 5 and 12 percent ( Barro and Lee, 2013 ; Soto, 2002 ) —a result that is in line with the micro-founded relationship between years of education and earnings ( Lovenheim and Smith, 2022 ).
To put this relationship in perspective and highlight the growth potential of increasing educational attainment, the CEA simulated the hypothetical effect on GDP of increasing the college-going rate by 1, 3, and 5 percentage points, respectively. This range represents the kinds of changes in college going that have been observed over several years: the college enrollment rate for 18- to 24-year-olds declined 4 percentage points between 2011 and 2021 after increasing by 6 percentage points between 2000 and 2011 ( NCES 2023 ). CEA simulations show that by 2055, a policy that increased the college going rate by 1, 3, and 5 percentage points could increase the level of GDP in 2055 (thirty years from now) by 0.2, 0.6, and 1 percent respectively. This represents hundreds of billions of dollars of additional economic activity in the long run.
While increased growth is an exciting possibility, it would only occur insofar as SAVE leads to increased educational attainment, which is uncertain. The academic literature has found that student loans can promote academic performance ( Barr, et. al. 2021 ), and increase educational attainment by increasing transfers from 2-year to 4-year colleges and increasing college completion among enrollees ( Marx and Turner, 2019 ). At the same time, increases in college-going due to SAVE are by no means guaranteed. While, historically, policies that reduce the cost of college through direct means—such as providing students with generous grant aid, or reducing tuition—have succeeded at raising college enrollment levels ( Dynarski, 2003 ; Turner, 2011 ), a pair of recent studies show that prospective students may only respond to cost changes when they are salient, i.e., they are framed and marketed in the right way ( Dynarski et al., 2021 ), and relatively certain ( Burland et al., 2022 ). However, evidence suggests that there is demand for plans like SAVE ( Balakrishnan et al., 2024 ), particularly as SAVE can provide sizable benefits to borrowers in terms of reducing their long-term debt burden and keep monthly payments low (dependent on a borrower’s income) after they finish school.
This highlights the importance of communicating the benefits of the SAVE program to prospective students who otherwise would not enroll in college due to cost concerns, including potential barriers to paying off student loans in the future. Doing so could lead to meaningful increases in college enrollment, and the resulting improvements in productive capacity could increase the size of the U.S. economy for years to come.
Concluding remarks
The Biden-Harris Administration has taken bold action to address a student debt problem that has been decades in the making. This student debt cancellation will provide well-deserved relief for borrowers who have paid their fair share, many of whom had the proverbial rug pulled out from under them with concurrent rapidly rising tuition and declining returns to a college degree. The relief has and will improve economic health and wellbeing of those who have devoted years of their life to public service, those who were defrauded or misled by their institutions, and those who have been doing all they can to make payments, but have still seen their loan balances grow. Looking to future generations, the Administration implemented the SAVE plan to protect borrowers against tuition spikes and poorer than expected labor market outcomes that often plague students graduating into a period of economic downturn ( Rothstein, 2021 ; Schwandt and von Wachter, 2023 ).
Both student debt relief and SAVE will enhance the economic status of millions of Americans with student debt: enable them to allocate more funds towards basic necessities, take career risks, start businesses, and purchase homes with the understanding that they will never have to pay more than they can afford towards their student loans. Moreover, the SAVE plan makes repayment more affordable for future generations, which helps borrowers manage monthly payments, but also enables more people from all walks of life to explore their full potential and pursue higher education, enhancing the potential of the U.S. workforce and the economy more broadly.
[1] In 2021, 51% of total undergraduates attended public 4-year universities and 21% attended public 2-years in 2021.
[2] The BA group excludes those with a graduate degree, or any education beyond a bachelor’s degree.
[3] Recent research shows that, despite a positive return on investment (ROI) for many, including the average student, the distribution of ROI has widened over the last several decades such that the likelihood of negative ROI is higher than it has historically been, particularly so for underrepresented minority students ( Webber 2022 ).
[4] There is also some evidence in support of the Bennett Hypothesis at the graduate level ( Black et al. 2023 ).
Stay Connected
We'll be in touch with the latest information on how President Biden and his administration are working for the American people, as well as ways you can get involved and help our country build back better.
Opt in to send and receive text messages from President Biden.
- SelectedWorks

- < Previous Event
- Next Event >
Home > MURC > 2024 > 17

The Effects of Covid-19 on Substance Use Among College Students
Presenter Information
Madison M. Wakely , Molloy University Follow Halle Trahey , Molloy University Follow Jennifer C. Elliott PhD , Molloy University Follow
Presenter Major
Presentation type.
Hays Theatre, Wilbur Arts Building
26-4-2024 10:45 AM
26-4-2024 11:30 AM
Description (Abstract)
Recent studies have shown mixed results on whether substance use has increased in college students over the course of the Coronavirus pandemic. This study surveyed 115 undergraduate students at a largely commuter college in the suburban northeast. The data suggested that mental health issues increased since before the pandemic, while alcohol use has largely stayed the same over the course of the pandemic. Continued research in diverse college settings is needed on this important topic.
Related Pillar(s)
This document is currently not available here.
Since April 17, 2024
- Call for Submissions
- Register to attend
Advanced Search
- Notify me via email or RSS
- Collections
- Disciplines
Author Corner
- Molloy Faculty Profiles
- DigitalCommons LibGuide
Home | About | FAQ | My Account | Accessibility Statement
Privacy Copyright
This paper is in the following e-collection/theme issue:
Published on 17.4.2024 in Vol 26 (2024)
Digital Interventions for Recreational Cannabis Use Among Young Adults: Systematic Review, Meta-Analysis, and Behavior Change Technique Analysis of Randomized Controlled Studies
Authors of this article:
- José Côté 1, 2, 3 , RN, PhD ;
- Gabrielle Chicoine 3, 4 , RN, PhD ;
- Billy Vinette 1, 3 , RN, MSN ;
- Patricia Auger 2, 3 , MSc ;
- Geneviève Rouleau 3, 5, 6 , RN, PhD ;
- Guillaume Fontaine 7, 8, 9 , RN, PhD ;
- Didier Jutras-Aswad 2, 10 , MSc, MD
1 Faculty of Nursing, Université de Montréal, Montreal, QC, Canada
2 Research Centre of the Centre Hospitalier de l’Université de Montréal, Montreal, QC, Canada
3 Research Chair in Innovative Nursing Practices, Montreal, QC, Canada
4 Knowledge Translation Program, Li Ka Shing Knowledge Institute, St. Michael’s Hospital, Toronto, ON, Canada
5 Department of Nursing, Université du Québec en Outaouais, Saint-Jérôme, QC, Canada
6 Women's College Hospital Institute for Health System Solutions and Virtual Care, Women's College Hospital, Toronto, ON, Canada
7 Ingram School of Nursing, Faculty of Medicine and Health Sciences, McGill University, Montreal, QC, Canada
8 Centre for Clinical Epidemiology, Lady Davis Institute for Medical Research, Sir Mortimer B. Davis Jewish General Hospital, Montreal, QC, Canada
9 Kirby Institute, University of New South Wales, Sydney, Australia
10 Department of Psychiatry and Addictology, Faculty of Medicine, Université de Montréal, Montreal, QC, Canada
Corresponding Author:
José Côté, RN, PhD
Research Centre of the Centre Hospitalier de l’Université de Montréal
850 Saint-Denis
Montreal, QC, H2X 0A9
Phone: 1 514 890 8000
Email: [email protected]
Background: The high prevalence of cannabis use among young adults poses substantial global health concerns due to the associated acute and long-term health and psychosocial risks. Digital modalities, including websites, digital platforms, and mobile apps, have emerged as promising tools to enhance the accessibility and availability of evidence-based interventions for young adults for cannabis use. However, existing reviews do not consider young adults specifically, combine cannabis-related outcomes with those of many other substances in their meta-analytical results, and do not solely target interventions for cannabis use.
Objective: We aimed to evaluate the effectiveness and active ingredients of digital interventions designed specifically for cannabis use among young adults living in the community.
Methods: We conducted a systematic search of 7 databases for empirical studies published between database inception and February 13, 2023, assessing the following outcomes: cannabis use (frequency, quantity, or both) and cannabis-related negative consequences. The reference lists of included studies were consulted, and forward citation searching was also conducted. We included randomized studies assessing web- or mobile-based interventions that included a comparator or control group. Studies were excluded if they targeted other substance use (eg, alcohol), did not report cannabis use separately as an outcome, did not include young adults (aged 16-35 y), had unpublished data, were delivered via teleconference through mobile phones and computers or in a hospital-based setting, or involved people with mental health disorders or substance use disorders or dependence. Data were independently extracted by 2 reviewers using a pilot-tested extraction form. Authors were contacted to clarify study details and obtain additional data. The characteristics of the included studies, study participants, digital interventions, and their comparators were summarized. Meta-analysis results were combined using a random-effects model and pooled as standardized mean differences.
Results: Of 6606 unique records, 19 (0.29%) were included (n=6710 participants). Half (9/19, 47%) of these articles reported an intervention effect on cannabis use frequency. The digital interventions included in the review were mostly web-based. A total of 184 behavior change techniques were identified across the interventions (range 5-19), and feedback on behavior was the most frequently used (17/19, 89%). Digital interventions for young adults reduced cannabis use frequency at the 3-month follow-up compared to control conditions (including passive and active controls) by −6.79 days of use in the previous month (95% CI −9.59 to −4.00; P <.001).
Conclusions: Our results indicate the potential of digital interventions to reduce cannabis use in young adults but raise important questions about what optimal exposure dose could be more effective, both in terms of intervention duration and frequency. Further high-quality research is still needed to investigate the effects of digital interventions on cannabis use among young adults.
Trial Registration: PROSPERO CRD42020196959; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=196959
Introduction
Cannabis use among young adults is recognized as a public health concern.
Young adulthood (typically the ages of 18-30 y) is a critical developmental stage characterized by a peak prevalence of substance use [ 1 , 2 ]. Worldwide, cannabis is a substance frequently used for nonmedical purposes due in part to its high availability in some regions and enhanced product variety and potency [ 3 , 4 ]. The prevalence of cannabis use (CU) among young adults is high [ 5 , 6 ], and its rates have risen in recent decades [ 7 ]. In North America and Oceania, the estimated past-year prevalence of CU is ≥25% among young adults [ 8 , 9 ].
While the vast majority of cannabis users do not experience severe problems from their use [ 4 ], the high prevalence of CU among young adults poses substantial global health concerns due to the associated acute and long-term health and psychosocial risks [ 10 , 11 ]. These include impairment of cognitive function, memory, and psychomotor skills during acute intoxication; increased engagement in behaviors with a potential for injury and fatality (eg, driving under the influence); socioeconomic problems; and diminished social functioning [ 4 , 12 - 14 ]. Importantly, an extensive body of literature reveals that subgroups engaging in higher-risk use, such as intensive or repeated use, are more prone to severe and chronic consequences, including physical ailments (eg, respiratory illness and reproductive dysfunction), mental health disorders (eg, psychosis, depression, and suicidal ideation or attempts), and the potential development of CU disorder [ 4 , 15 - 17 ].
Interventions to Reduce Public Health Impact of Young Adult CU
Given the increased prevalence of lifetime and daily CU among young adults and the potential negative impact of higher-risk CU, various prevention and intervention programs have been implemented to help users reduce or cease their CU. These programs primarily target young adults regardless of their CU status [ 2 , 18 ]. In this context, many health care organizations and international expert panels have developed evidence-based lower-risk CU guidelines to promote safer CU and intervention options to help reduce risks of adverse health outcomes from nonmedical CU [ 4 , 16 , 17 , 19 ]. Lower-risk guidance-oriented interventions for CU are based on concepts of health promotion [ 20 - 22 ] and health behavior change [ 23 - 26 ] and on other similar harm reduction interventions implemented in other areas of population health (eg, lower-risk drinking guidelines, supervised consumption sites and services, and sexual health) [ 27 , 28 ]. These interventions primarily aim to raise awareness of negative mental, physical, and social cannabis-related consequences to modify individual-level behavior-related risk factors.
Meta-analyses have shown that face-to-face prevention and treatment interventions are generally effective in reducing CU in young adults [ 18 , 29 - 32 ]. However, as the proportion of professional help seeking for CU concerns among young adults remains low (approximately 15%) [ 33 , 34 ], alternative strategies that consider the limited capacities and access-related barriers of traditional face-to-face prevention and treatment facilities are needed. Digital interventions, including websites, digital platforms, and mobile apps, have emerged as promising tools to enhance the accessibility and availability of evidence-based programs for young adult cannabis users. These interventions address barriers such as long-distance travel, concerns about confidentiality, stigma associated with seeking treatment, and the cost of traditional treatments [ 35 - 37 ]. By overcoming these barriers, digital interventions have the potential to have a stronger public health impact [ 18 , 38 ].
State of Knowledge of Digital Interventions for CU and Young Adults
The literature regarding digital interventions for substance use has grown rapidly in the past decade, as evidenced by several systematic reviews and meta-analyses of randomized controlled trial (RCT) studies on the efficacy or effectiveness of these interventions in preventing or reducing harmful substance use [ 2 , 39 - 41 ]. However, these reviews do not focus on young adults specifically. In addition, they combine CU-related outcomes with those of many other substances in their meta-analytical results. Finally, they do not target CU interventions exclusively.
In total, 4 systematic reviews and meta-analyses of digital interventions for CU among young people have reported mixed results [ 42 - 45 ]. In their systematic review (10 studies of 5 prevention and 5 treatment interventions up to 2012), Tait et al [ 44 ] concluded that digital interventions effectively reduced CU among adolescents and adults at the posttreatment time point. Olmos et al [ 43 ] reached a similar conclusion in their meta-analysis of 9 RCT studies (2 prevention and 7 treatment interventions). In their review, Hoch et al [ 42 ] reported evidence of small effects at the 3-month follow-up based on 4 RCTs of brief motivational interventions and cognitive behavioral therapy (CBT) delivered on the web. In another systematic review and meta-analysis, Beneria et al [ 45 ] found that web-based CU interventions did not significantly reduce consumption. However, these authors indicated that the programs tested varied significantly across the studies considered and that statistical heterogeneity was attributable to the inclusion of studies of programs targeting more than one substance (eg, alcohol and cannabis) and both adolescents and young adults. Beneria et al [ 45 ] recommend that future work “establish the effectiveness of the newer generation of interventions as well as the key ingredients” of effective digital interventions addressing CU by young people. This is of particular importance because behavior change interventions tend to be complex as they consist of multiple interactive components [ 46 ].
Behavior change interventions refer to “coordinated sets of activities designed to change specified behavior patterns” [ 47 ]. Their interacting active ingredients can be conceptualized as behavior change techniques (BCTs) [ 48 ]. BCTs are specific and irreducible. Each BCT has its own individual label and definition, which can be used when designing and reporting complex interventions and as a nomenclature system when coding interventions for their content [ 47 ]. The Behavior Change Technique Taxonomy version 1 (BCTTv1) [ 48 , 49 ] was developed to provide a shared, standardized terminology for characterizing complex behavior change interventions and their active ingredients. Several systematic reviews with meta-regressions that used the BCTTv1 have found interventions with certain BCTs to be more effective than those without [ 50 - 53 ]. A better understanding of the BCTs used in digital interventions for young adult cannabis users would help not only to establish the key ingredients of such interventions but also develop and evaluate effective interventions.
In the absence of any systematic review of the effectiveness and active ingredients of digital interventions designed specifically for CU among community-living young adults, we set out to achieve the following:
- conduct a comprehensive review of digital interventions for preventing, reducing, or ceasing CU among community-living young adults,
- describe the active ingredients (ie, BCTs) in these interventions from the perspective of behavior change science, and
- analyze the effectiveness of these interventions on CU outcomes.
Protocol Registration
We followed the Cochrane Handbook for Systematic Reviews of Interventions [ 54 ] in designing this systematic review and meta-analysis and the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines in reporting our findings (see Multimedia Appendix 1 [ 55 ] for the complete PRISMA checklist). This review was registered in PROSPERO (CRD42020196959).
Search Strategy
The search strategy was designed by a health information specialist together with the research team and peer reviewed by another senior information specialist before execution using Peer Review of Electronic Search Strategies for systematic reviews [ 56 ]. The search strategy revolved around three concepts:
- CU (eg, “cannabis,” “marijuana,” and “hashish”)
- Digital interventions (eg, “telehealth,” “website,” “mobile applications,” and “computer”)
- Young adults (eg, “emerging adults” and “students”)
The strategy was initially implemented on March 18, 2020, and again on October 13, 2021, and February 13, 2023. The full, detailed search strategies for each database are presented in Multimedia Appendix 2 .
Information Sources
We searched 7 electronic databases of published literature: CINAHL Complete, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Embase, MEDLINE, PubMed, and PsycINFO. No publication date filters or language restrictions were applied. A combination of free-text keywords and Medical Subject Headings was tailored to the conventions of each database for optimal electronic searching. The research team also manually screened the reference lists of the included articles and the bibliographies of existing systematic reviews [ 18 , 31 , 42 - 45 ] to identify additional relevant studies (snowballing). Finally, a forward citation tracking procedure (ie, searching for articles that cited the included studies) was carried out in Google Scholar.
Inclusion Criteria
The population, intervention, comparison, outcome, and study design process is presented in Multimedia Appendix 3 . The inclusion criteria were as follows: (1) original research articles published in peer-reviewed journals; (2) use of an experimental study design (eg, RCT, cluster RCT, or pilot RCT); (3) studies evaluating the effectiveness (or efficacy) of digital interventions designed specifically to prevent, reduce, or cease CU as well as promote CU self-management or address cannabis-related harm and having CU as an outcome measure; (4) studies targeting young adults, including active and nonactive cannabis users; (5) cannabis users and nonusers not under substance use treatment used as controls in comparator, waitlist, or delayed-treatment groups offered another type of intervention (eg, pharmacotherapy or psychosocial) different from the one being investigated or participants assessed only for CU; and (6) quantitative CU outcomes (frequency and quantity) or cannabis abstinence. Given the availability of numerous CU screening and assessment tools with adequate psychometric properties and the absence of a gold standard in this regard [ 57 ], any instrument capturing aspects of CU was considered. CU outcome measures could be subjective (eg, self-reported number of CU days or joints in the previous 3 months) or objective (eg, drug screening test). CU had to be measured before the intervention (baseline) and at least once after.
Digital CU interventions were defined as web- or mobile-based interventions that included one or more activities (eg, self-directed or interactive psychoeducation or therapy, personalized feedback, peer-to-peer contact, and patient-to-expert communication) aimed at changing CU [ 58 ]. Mobile-based interventions were defined as interventions delivered via mobile phone through SMS text message, multimedia messaging service (ie, SMS text messages that include multimedia content, such as pictures, videos, or emojis), or mobile apps, whereas web-based interventions (eg, websites and digital platforms) were defined as interventions designed to be accessed on the web (ie, the internet), mainly via computers. Interventions could include self-directed and web-based interventions with human support. We defined young adults as aged 16 to 35 years and included students and nonstudents. While young adulthood is typically defined as covering the ages of 18 to 30 years [ 59 ], we broadened the range given that the age of majority and legal age to purchase cannabis differs across countries and jurisdictions. This was also in line with the age range targeted by several digital CU interventions (college or university students or emerging adults aged 15-24 years) [ 31 , 45 ]. Given the language expertise of the research team members and the available resources, only English- and French-language articles were retained.
Exclusion Criteria
Knowledge synthesis articles, study protocols, and discussion papers or editorials were excluded, as were articles with cross-sectional, cohort, case study or report, pretest-posttest, quasi-experimental, or qualitative designs. Mixed methods designs were included only if the quantitative component was an RCT. We excluded studies if (1) use of substances other than cannabis (eg, alcohol, opioids, or stimulants) was the focus of the digital intervention (though studies that included polysubstance users were retained if CU was assessed and reported separately); (2) CU was not reported separately as an outcome or only attitudes or beliefs regarding, knowledge of, intention to reduce, or readiness or motivation to change CU was measured; and (3) the data reported were unpublished (eg, conferences and dissertations). Studies of traditional face-to-face therapy delivered via teleconference on mobile phones and computers or in a hospital-based setting and informational campaigns (eg, web-based poster presentations or pamphlets) were excluded as well. Studies with samples with a maximum age of <15 years and a minimum age of >35 years were also excluded. Finally, we excluded studies that focused exclusively on people with a mental health disorder or substance use disorder or dependence or on adolescents owing to the particular health care needs of these populations, which may differ from those of young adults [ 1 ].
Data Collection
Selection of studies.
Duplicates were removed from the literature search results in EndNote (version X9.3.3; Clarivate Analytics) using the Bramer method for deduplication of database search results for systematic reviews [ 60 ]. The remaining records were uploaded to Covidence (Veritas Health Innovation), a web-based systematic review management system. A reviewer guide was developed that included screening questions and a detailed description of each inclusion and exclusion criterion based on PICO (population, intervention, comparator, and outcome), and a calibration exercise was performed before each stage of the selection process to maximize consistency between reviewers. Titles and abstracts of studies flagged for possible inclusion were screened first by 2 independent reviewers (GC, BV, PA, and GR; 2 per article) against the eligibility criteria (stage 1). Articles deemed eligible for full-text review were then retrieved and screened for inclusion (stage 2). Full texts were assessed in detail against the eligibility criteria again by 2 reviewers independently. Disagreements between reviewers were resolved through consensus or by consulting a third reviewer.
Data Extraction Process
In total, 2 reviewers (GC, BV, PA, GR, and GF; 2 per article) independently extracted relevant data (or informal evidence) using a data extraction form developed specifically for this review and integrated into Covidence. The form was pilot-tested on 2 randomly selected studies and refined accordingly. Data pertaining to the following domains were extracted from the included studies: (1) Study characteristics included information on the first and corresponding authors, publication year, country of origin, aims and hypotheses, study period, design (including details on randomization and blinding), follow-up times, data collection methods, and types of statistical analysis. (2) Participant characteristics included study target population, participant inclusion and exclusion criteria, sex or gender, mean age, and sample sizes at each data collection time point. (3) Intervention characteristics, for which the research team developed a matrix inspired by the template for intervention description and replication 12-item checklist [ 61 ] to extract informal evidence (ie, intervention descriptions) from the included studies under the headings name of intervention, purpose, underpinning theory of design elements, treatment approach, type of technology (ie, web or mobile) and software used, delivery format (ie, self-directed, human involvement, or both), provider characteristics (if applicable), intervention duration (ie, length of treatment and number of sessions or modules), material and procedures (ie, tools or activities offered, resources provided, and psychoeducational content), tailoring, and unplanned modifications. (4) Comparator characteristics were details of the control or comparison group or groups, including nature (passive vs active), number of groups or clusters (if applicable), type and length of the intervention (if applicable), and number of participants at each data collection time point. (5) Outcome variables, including the primary outcome variable examined in this systematic review, that is, the mean difference in CU frequency before and after the intervention and between the experimental and control or comparison groups. When possible, we examined continuous variables, including CU frequency means and SDs at the baseline and follow-up time points, and standardized regression coefficients (ie, β coefficients and associated 95% CIs). The secondary outcomes examined included other CU outcome variables (eg, quantity of cannabis used and abstinence) and cannabis-related negative consequences (or problems). Details on outcome variables (ie, definition, data time points, and missing data) and measurements (ie, instruments, measurement units, and scales) were also extracted.
In addition, data on user engagement and use of the digital intervention and study attrition rates (ie, dropouts and loss to follow-up) were extracted. When articles had missing data, we contacted the corresponding authors via email (2 attempts were made over a 2-month period) to obtain missing information. Disagreements over the extracted data were limited and resolved through discussion.
Data Synthesis Methods
Descriptive synthesis.
The characteristics of the included studies, study participants, interventions, and comparators were summarized in narrative and table formats. The template for intervention description and replication 12-item checklist [ 61 ] was used to summarize and organize intervention characteristics and assess to what extent the interventions were appropriately described in the included articles. As not all studies had usable data for meta-analysis purposes and because of heterogeneity, we summarized the main findings (ie, intervention effects) of the included studies in narrative and table formats for each outcome of interest in this review.
The BCTs used in the digital interventions were identified from the descriptions of the interventions (ie, experimental groups) provided in the articles as well as any supplementary material and previously published research protocols. A BCT was defined as “an observable, replicable, and irreducible component of an intervention designed to alter or redirect causal processes that regulate behavior” [ 48 ]. The target behavior in this review was the cessation or reduction of CU by young adults. BCTs were identified and coded using the BCTTv1 [ 48 , 49 ], a taxonomy of 93 BCTs organized into 16 hierarchical thematic clusters or categories. Applying the BCTTv1 in a systematic review allows for the comparison and synthesis of evidence across studies in a structured manner. This analysis allows for the identification of the explicit mechanisms underlying the reported behavior change induced by interventions, successful or not, and, thus, avoids making implicit assumptions about what works [ 62 ].
BCT coding was performed by 2 reviewers independently—BV coded all studies, and GC and GF coded a subset of the studies. All reviewers completed web-based training on the BCTTv1, and GF is an experienced implementation scientist who had used the BCTTv1 in prior work [ 63 - 65 ]. The descriptions of the interventions in the articles were read line by line and analyzed for the clear presence of BCTs using the guidelines developed by Michie et al [ 48 ]. For each article, the BCTs identified were documented and categorized using supporting textual evidence. They were coded only once per article regardless of how many times they came up in the text. Disagreements about including a BCT were resolved through discussion. If there was uncertainty about whether a BCT was present, it was coded as absent. Excel (Microsoft Corp) was used to compare the reviewers’ independent BCT coding and generate an overall descriptive synthesis of the BCTs identified. The BCTs were summarized by study and BCT cluster.
Statistical Analysis
Meta-analyses were conducted to estimate the size of the effect of the digital interventions for young adult CU on outcomes of interest at the posttreatment and follow-up assessments compared with control or alternative intervention conditions. The outcome variables considered were (1) CU frequency and other CU outcome variables (eg, quantity of cannabis used and abstinence) at baseline and the posttreatment time point or follow-up measured using standardized instruments of self-reported CU (eg, the timeline followback [TLFB] method) [ 66 ] and (2) cannabis-related negative consequences measured using standardized instruments (eg, the Marijuana Problems Scale) [ 67 ].
Under our systematic review protocol, ≥2 studies were needed for a meta-analysis. On the basis of previous systematic reviews and meta-analyses in the field of digital CU interventions [ 31 , 42 - 45 ], we expected between-study heterogeneity regarding outcome assessment. To minimize heterogeneity, we chose to pool studies with similar outcomes of interest based on four criteria: (1) definition of outcome (eg, CU frequency, quantity consumed, and abstinence), (2) type of outcome variable (eg, days of CU in the previous 90 days, days high per week in the previous 30 days, and number of CU events in the previous month) and measure (ie, instruments or scales), (3) use of validated instruments, and (4) posttreatment or follow-up time points (eg, 2 weeks or 1 month after the baseline or 3, 6, and 12 months after the baseline).
Only articles that reported sufficient statistics to compute a valid effect size with 95% CIs were included in the meta-analyses. In the case of articles that were not independent (ie, more than one published article reporting data from the same clinical trial), only 1 was included, and it was represented only once in the meta-analysis for a given outcome variable regardless of whether the data used to compute the effect size were extracted from the original paper or a secondary analysis paper. We made sure that the independence of the studies included in the meta-analysis of each outcome was respected. In the case of studies that had more than one comparator, we used the effect size for each comparison between the intervention and control groups.
Meta-analyses were conducted only for mean differences based on the change from baseline in CU frequency at 3 months after the baseline as measured using the number of self-reported days of use in the previous month. As the true value of the estimated effect size for outcome variables might vary across different trials and samples, we used a random-effects model given that the studies retained did not have identical target populations. The random-effects model incorporates between-study variation in the study weights and estimated effect size [ 68 ]. In addition, statistical heterogeneity across studies was assessed using I 2 , which measures the proportion of heterogeneity to the total observed dispersion; 25% was considered low, 50% was considered moderate, and 75% was considered high [ 69 ]. Because only 3 studies were included in the meta-analysis [ 70 - 72 ], publication bias could not be assessed. All analyses were completed using Stata (version 18; StataCorp) [ 73 ].
Risk-of-Bias Assessment
The risk of bias (RoB) of the included RCTs was assessed using the Cochrane RoB 2 tool at the outcome level [ 74 ]. Each distinct risk domain (ie, randomization process, deviations from the intended intervention, missing outcome data, measurement of the outcome, and selection of the reported results) was assessed as “low,” “some concerns,” or “high” based on the RoB 2 criteria. In total, 2 reviewers (GC and BV) conducted the assessments independently. Disagreements were discussed, and if not resolved consensually by the 2, the matter was left for a third reviewer (GF) to settle. The assessments were summarized by risk domain and outcome and converted into figures using the RoB visualization tool robvis [ 75 ].
Search Results
The database search generated a total of 13,232 citations, of which 7822 (59.11%) were from the initial search on March 18, 2020, and 2805 (21.2%) and 2605 (19.69%) were from the updates on October 13, 2021, and February 13, 2023, respectively. Figure 1 presents the PRISMA study flow diagram [ 76 ]. Of the 6606 unique records, 6484 (98.15%) were excluded based on title and abstract screening. Full texts of the remaining 1.85% (122/6606) of the records were examined, as were those of 25 more reports found through hand searching. Of these 147 records, 128 (87.1%) were excluded after 3 rounds of full-text screening. Of these 128 records, 39 (30.5%) were excluded for not being empirical research articles (eg, research protocols). Another 28.1% (36/128) were excluded for not meeting our definition of digital CU intervention. The remaining records were excluded for reasons that occurred with a frequency of ≤14%, including young adults not being the target population and the study not meeting our study design criteria (ie, RCT, cluster RCT, or pilot RCT). Excluded studies and reasons for exclusion are listed in Multimedia Appendix 4 . Finally, 19 articles detailing the results of 19 original studies were included.

Description of Studies
Study characteristics.
Multimedia Appendix 5 [ 70 - 72 , 77 - 92 ] describes the general characteristics of the 19 included studies. The studies were published between 2010 and 2023, with 58% (11/19) published in 2018 or later. A total of 53% (10/19) of the studies were conducted in the United States [ 77 - 86 ], 11% (2/19) were conducted in Canada [ 87 , 88 ], 11% (2/19) were conducted in Australia [ 71 , 89 ], 11% (2/19) were conducted in Germany [ 72 , 90 ], 11% (2/19) were conducted in Switzerland [ 70 , 91 ], and 5% (1/19) were conducted in Sweden [ 92 ]. A total of 79% (15/19) were RCTs [ 70 - 72 , 77 , 79 , 81 - 83 , 86 - 92 ], and 21% (4/19) were pilot RCTs [ 78 , 80 , 84 , 85 ].
Participant Characteristics
The studies enrolled a total of 6710 participants—3229 (48.1%) in the experimental groups, 3358 (50%) in the control groups, and the remaining 123 (1.8%) from 1 study [ 82 ] where participant allocation to the intervention condition was not reported. Baseline sample sizes ranged from 49 [ 81 ] to 1292 [ 72 ] (mean 352.89, SD 289.50), as shown in Multimedia Appendix 5 . Participant mean ages ranged from 18.03 (SD 0.31) [ 79 ] to 35.3 (SD 12.6) years [ 88 ], and the proportion of participants who identified as female ranged from 24.7% [ 91 ] to 84.1% [ 80 ].
Of the 19 included studies, 10 (53%) targeted adults aged ≥18 years, of which 7 (70%) studies focused on adults who had engaged in past-month CU [ 70 , 71 , 80 , 84 , 85 , 90 , 91 ], 2 (20%) studies included adults who wished to reduce or cease CU [ 72 , 89 ], and 1 (10%) study focused on noncollege adults with a moderate risk associated with CU [ 88 ]. Sinadinovic et al [ 92 ] targeted young adults aged ≥16 years who had used cannabis at least once a week in the previous 6 months. The remaining 8 studies targeted college or university students (aged ≥17 y) specifically, of which 7 (88%) studies focused solely on students who reported using cannabis [ 78 , 79 , 81 - 83 , 86 , 87 ] and 1 (12%) study focused solely on students who did not report past-month CU (ie, abstainers) [ 77 ].
Intervention Characteristics
The 19 included studies assessed nine different digital interventions: (1) 5 (26%) evaluated Marijuana eCHECKUP TO GO (e-TOKE), a commercially available electronic intervention used at colleges throughout the United States and Canada [ 77 , 78 , 81 - 83 ]; (2) 2 (11%) examined the internationally known CANreduce program [ 70 , 91 ]; (3) 2 (11%) evaluated the German Quit the Shit program [ 72 , 90 ]; (4) 2 (11%) assessed a social media–delivered, physical activity–focused cannabis intervention [ 84 , 85 ]; (5) 1 (5%) investigated the Swedish Cannabishjälpen intervention [ 92 ]; (6) 1 (5%) evaluated the Australian Grassessment: Evaluate Your Use of Cannabis website program [ 89 ]; (7) 1 (5%) assessed the Canadian Ma réussite, mon choix intervention [ 87 ]; (8) 1 (5%) examined the Australian Reduce Your Use: How to Break the Cannabis Habit program [ 71 ]; and (9) 4 (21%) each evaluated a unique no-name intervention described as a personalized feedback intervention (PFI) [ 79 , 80 , 86 , 88 ]. Detailed information regarding the characteristics of all interventions as reported in each included study is provided in Multimedia Appendix 6 [ 70 - 72 , 77 - 113 ] and summarized in the following paragraphs.
In several studies (8/19, 42%), the interventions were designed to support cannabis users in reducing or ceasing their consumption [ 70 , 72 , 80 , 87 , 89 - 92 ]. In 37% (7/19) of the studies, the interventions aimed at reducing both CU and cannabis-related consequences [ 79 , 81 - 85 , 88 ]. Other interventions focused on helping college students think carefully about the decision to use cannabis [ 77 , 78 ] and on reducing either cannabis-related problems among undergraduate students [ 86 ] or symptoms associated with CU disorder in young adults [ 71 ].
In 26% (5/19) of the studies, theory was used to inform intervention design along with a clear rationale for theory use. Of these 5 articles, only 1 (20%) [ 87 ] reported using a single theory of behavior change, the theory of planned behavior [ 114 ]. A total of 21% (4/19) of the studies selected only constructs of theories (or models) for their intervention design. Of these 4 studies, 2 (50%) evaluated the same intervention [ 72 , 90 ], which focused on principles of self-regulation and self-control theory [ 93 ]; 1 (25%) [ 70 ] used the concept of adherence-focused guidance enhancement based on the supportive accountability model of guidance [ 94 ]; and 1 (25%) [ 71 ] reported that intervention design was guided by the concept of self-behavioral management.
The strategies (or approaches) used in the delivery of the digital interventions were discussed in greater detail in 84% (16/19) of the articles [ 70 - 72 , 79 - 81 , 83 - 92 ]. Many of these articles (9/19, 47%) reported using a combination of approaches based on CBT or motivational interviewing (MI) [ 70 , 71 , 79 , 83 - 85 , 90 - 92 ]. PFIs were also often mentioned as an approach to inform intervention delivery [ 7 , 71 , 79 , 86 - 88 ].
More than half (13/19, 68%) of all the digital interventions were asynchronous and based on a self-guided approach without support from a counselor or therapist. The study by Côté et al [ 87 ] evaluated the efficacy of a web-based tailored intervention focused on reinforcing a positive attitude toward and a sense of control over cannabis abstinence through psychoeducational messages delivered by a credible character in short video clips and personalized reinforcement messages. Lee et al [ 79 ] evaluated a brief, web-based personalized feedback selective intervention based on the PFI approach pioneered by Marlatt et al [ 95 ] for alcohol use prevention and on the MI approach described by Miller and Rollnick [ 96 ]. Similarly, Rooke et al [ 71 ] combined principles of MI and CBT to develop a web-based intervention delivered via web modules, which were informed by previous automated feedback interventions targeting substance use. The study by Copeland et al [ 89 ] assessed the short-term effectiveness of Grassessment: Evaluate Your Use of Cannabis, a brief web-based, self-complete intervention based on motivational enhancement therapy that included personalized feedback messages and psychoeducational material. In the studies by Buckner et al [ 80 ], Cunningham et al [ 88 ], and Walukevich-Dienst et al [ 86 ], experimental groups received a brief web-based PFI available via a computer. A total of 16% (3/19) of the studies [ 77 , 78 , 82 ] applied a program called the Marijuana eCHECKUP TO GO (e-TOKE) for Universities and Colleges, which was presented as a web-based, norm-correcting, brief preventive and intervention education program designed to prompt self-reflection on consequences and consideration of decreasing CU among students. Riggs et al [ 83 ] developed and evaluated an adapted version of e-TOKE that provided participants with university-specific personalized feedback and normative information based on protective behavioral strategies for CU [ 97 ]. Similarly, Goodness and Palfai [ 81 ] tested the efficacy of eCHECKUP TO GO-cannabis, a modified version of e-TOKE combining personalized feedback, norm correction, and a harm and frequency reduction strategy where a “booster” session was provided at 3 months to allow participants to receive repeated exposure to the intervention.
In the remaining 32% (6/19) of the studies, which examined 4 different interventions, the presence of a therapist guide was reported. The intervention evaluated by Sinadinovic et al [ 92 ] combined principles of psychoeducation, MI, and CBT organized into 13 web-based modules and a calendar involving therapist guidance, recommendations, and personal feedback. In total, 33% (2/6) of these studies evaluated a social media–delivered intervention with e-coaches that combined principles of MI and CBT and a harm reduction approach for risky CU [ 84 , 85 ]. Schaub et al [ 91 ] evaluated the efficacy of CANreduce, a web-based self-help intervention based on both MI and CBT approaches, using automated motivational and feedback emails, chat with a counselor, and web-based psychoeducational modules. Similarly, Baumgartner et al [ 70 ] investigated the effectiveness of CANreduce 2.0, a modified version of CANreduce, using semiautomated motivational and adherence-focused guidance-based email feedback with or without a personal online coach. The studies by Tossman et al [ 72 ] and Jonas et al [ 90 ] used a solution-focused approach and MI to evaluate the effectiveness of the German Quit the Shit web-based program that involves weekly feedback provided by counselors.
In addition to using different intervention strategies or approaches, the interventions were diverse in terms of the duration and frequency of the program (eg, web-based activities, sessions, or modules). Of the 12 articles that provided details in this regard, 2 (17%) on the same intervention described it as a brief 20- to 45-minute web-based program [ 77 , 78 ], 2 (17%) on 2 different interventions reported including 1 or 2 modules per week for a duration of 6 weeks [ 71 , 92 ], and 7 (58%) on 4 different interventions described them as being available over a longer period ranging from 6 weeks to 3 months [ 70 , 72 , 79 , 84 , 85 , 87 , 90 , 91 ].
Comparator Types
A total of 42% (8/19) of the studies [ 72 , 77 - 80 , 85 , 87 , 92 ] used a passive comparator only, namely, a waitlist control group ( Multimedia Appendix 5 ). A total of 26% (5/19) of the studies used an active comparator only where participants were provided with minimal general health feedback regarding recommended guidelines for sleep, exercise, and nutrition [ 81 , 82 ]; strategies for healthy stress management [ 83 ]; educational materials about risky CU [ 88 ]; or access to a website containing information about cannabis [ 71 ]. In another 21% (4/19) of the studies, which used an active comparator, participants received the same digital intervention minus a specific component: a personal web-based coach [ 70 ], extended personalized feedback [ 89 ], web-based chat counseling [ 91 ], or information on risks associated with CU [ 86 ]. A total of 21% (4/19) of the studies had more than one control group [ 70 , 84 , 90 , 91 ].
Outcome Variable Assessment and Summary of Main Findings of the Studies
The methodological characteristics and major findings of the included studies (N=19) are presented in Multimedia Appendix 7 [ 67 , 70 - 72 , 77 - 92 , 115 - 120 ] and summarized in the following sections for each outcome of interest in this review (ie, CU and cannabis-related consequences). Of the 19 studies, 11 (58%) were reported as efficacy trials [ 7 , 77 , 79 , 81 - 83 , 86 - 88 , 91 , 92 ], and 8 (42%) were reported as effectiveness trials [ 70 - 72 , 78 , 84 , 85 , 89 , 90 ].
Across all the included studies (19/19, 100%), participant attrition rates ranged from 1.6% at 1 month after the baseline [ 77 , 78 ] to 75.1% at the 3-month follow-up [ 70 ]. A total of 37% (7/19) of the studies assessed and reported results regarding user engagement [ 71 , 78 , 84 , 85 , 90 - 92 ] using different types of metrics. In one article on the Marijuana eCHECKUP TO GO (e-TOKE) web-based program [ 78 ], the authors briefly reported that participation was confirmed for 98.1% (158/161) of participants in the intervention group. In 11% (2/19) of the studies, which were on a similar social media–delivered intervention [ 84 , 85 ], user engagement was quantified by tallying the number of comments or posts and reactions (eg, likes and hearts) left by participants. In both studies [ 84 , 85 ], the intervention group, which involved a CU-related Facebook page, displayed greater interactions than the control groups, which involved a Facebook page unrelated to CU. One article [ 84 ] reported that 80% of participants in the intervention group posted at least once (range 0-60) and 50% posted at least weekly. In the other study [ 85 ], the results showed that intervention participants engaged (ie, posting or commenting or clicking reactions) on average 47.9 times each over 8 weeks. In total, 11% (2/19) of the studies [ 90 , 91 ] on 2 different web-based intervention programs, both consisting of web documentation accompanied by chat-based counseling, measured user engagement either by average duration or average number of chat sessions. Finally, 16% (3/19) of the studies [ 71 , 91 , 92 ], which involved 3 different web-based intervention programs, characterized user engagement by the mean number of web modules completed per participant. Overall, the mean number of web modules completed reported in these articles was quite similar: 3.9 out of 13 [ 92 ] and 3.2 [ 91 ] and 3.5 [ 71 ] out of 6.
Assessment of CU
As presented in Multimedia Appendix 7 , the included studies differed in terms of how they assessed CU, although all used at least one self-reported measure of frequency. Most studies (16/19, 84%) measured frequency by days of use, including days of use in the preceding week [ 91 ] or 2 [ 80 ], days of use in the previous 30 [ 70 - 72 , 78 , 84 - 86 , 88 - 90 ] or 90 days [ 79 , 81 , 82 ], and days high per week [ 83 ]. Other self-reported measures of CU frequency included (1) number of CU events in the previous month [ 87 , 90 ], (2) cannabis initiation or use in the previous month (ie, yes or no) [ 77 ], and (3) days without CU in the previous 7 days [ 92 ]. In addition to measuring CU frequency, 42% (8/19) of the studies also assessed CU via self-reported measures of quantity used, including estimated grams consumed in the previous week [ 92 ] or 30 days [ 72 , 85 , 90 ] and the number of standard-sized joints consumed in the previous 7 days [ 91 ] or the previous month [ 70 , 71 , 89 ].
Of the 19 articles included, 10 (53%) [ 70 - 72 , 80 , 84 - 86 , 89 , 90 , 92 ] reported using a validated instrument to measure CU frequency or quantity, including the TLFB instrument [ 66 ] (n=9, 90% of the studies) and the Marijuana Use Form (n=1, 10% of the studies); 1 (10%) [ 79 ] reported using CU-related questions from an adaptation of the Global Appraisal of Individual Needs–Initial instrument [ 115 ]; and 30% (3/10) [ 81 , 82 , 91 ] reported using a questionnaire accompanied by a calendar or a diary of consumption. The 19 studies also differed with regard to their follow-up time measurements for assessing CU, ranging from 2 weeks after the baseline [ 80 ] to 12 months after randomization [ 90 ], although 12 (63%) of the studies included a 3-month follow-up assessment [ 70 - 72 , 79 , 81 , 82 , 84 , 85 , 88 , 90 - 92 ].
Of all studies assessing and reporting change in CU frequency from baseline to follow-up assessments (19/19, 100%), 47% (9/19) found statistically significant differences between the experimental and control groups [ 70 - 72 , 80 , 81 , 83 , 85 , 87 , 91 ]. Importantly, 67% (6/9) of these studies showed that participants in the experimental groups exhibited greater decreases in CU frequency 3 months following the baseline assessment compared with participants in the control groups [ 70 - 72 , 81 , 85 , 91 ], 22% (2/9) of the studies showed greater decreases in CU frequency at 6 weeks after the baseline assessment [ 71 , 83 ], 22% (2/9) of the studies showed greater decreases in CU frequency at 6 months following the baseline assessment [ 81 , 85 ], 11% (1/9) of the studies showed greater decreases in CU frequency at 2 weeks after the baseline [ 80 ], and 11% (1/9) of the studies showed greater decreases in CU frequency at 2 months after treatment [ 87 ].
In the study by Baumgartner et al [ 70 ], a reduction in CU days was observed in all groups, but the authors reported that the difference was statistically significant only between the intervention group with the service team and the control group (the reduction in the intervention group with social presence was not significant). In the study by Bonar et al [ 85 ], the only statistically significant difference between the intervention and control groups at the 3- and 6-month follow-ups involved total days of cannabis vaping in the previous 30 days. Finally, in the study by Buckner et al [ 80 ], the intervention group had less CU than the control group 2 weeks after the baseline; however, this was statistically significant only for participants with moderate or high levels of social anxiety.
Assessment of Cannabis-Related Negative Consequences
A total of 53% (10/19) of the studies also assessed cannabis-related negative consequences [ 78 - 84 , 86 , 88 , 92 ]. Of these 10 articles, 8 (80%) reported using a validated self-report instrument: 4 (50%) [ 81 , 82 , 86 , 88 ] used the 19-item Marijuana Problems Scale [ 67 ], 2 (25%) [ 78 , 79 ] used the 18-item Rutgers Marijuana Problem Index [ 121 , 122 ], and 2 (25%) [ 80 , 84 ] used the Brief Marijuana Consequences Questionnaire [ 116 ]. Only 10% (1/10) of the studies [ 92 ] used a screening tool, the Cannabis Abuse Screening Test [ 117 , 118 ]. None of these 10 studies demonstrated a statistically significant difference between the intervention and control groups. Of note, Walukevich-Dienst et al [ 86 ] found that women (but not men) who received an web-based PFI with additional information on CU risks reported significantly fewer cannabis-related problems than did women in the control group at 1 month after the intervention ( B =−1.941; P =.01).
Descriptive Summary of BCTs Used in Intervention Groups
After the 19 studies included in this review were coded, a total of 184 individual BCTs targeting CU in young adults were identified. Of these 184 BCTs, 133 (72.3% ) were deemed to be present beyond a reasonable doubt, and 51 (27.7%) were deemed to be present in all probability. Multimedia Appendix 8 [ 48 , 70 - 72 , 77 - 92 ] presents all the BCTs coded for each included study summarized by individual BCT and BCT cluster.
The 184 individual BCTs coded covered 38% (35/93) of the BCTs listed in the BCTTv1 [ 48 ]. The number of individual BCTs identified per study ranged from 5 to 19, with two-thirds of the 19 studies (12/19, 63%) using ≤9 BCTs (mean 9.68). As Multimedia Appendix 8 shows, at least one BCT fell into 13 of the 16 possible BCT clusters. The most frequent clusters were feedback monitoring , natural consequences , goal planning , and comparison of outcomes .
The most frequently coded BCTs were (1) feedback on behavior (BCT 2.2; 17/19, 89% of the studies; eg, “Once a week, participants receive detailed feedback by their counselor on their entries in diary and exercises. Depending on the involvement of each participant, up to seven feedbacks are given” [ 90 ]), (2) social support (unspecified) (BCT 3.1; 15/19, 79% of the studies; eg, “The website also features [...] blogs from former cannabis users, quick assist links, and weekly automatically generated encouragement emails” [ 71 ]), and (3) pros and cons (BCT 9.2; 14/19, 74% of the studies; eg, “participants are encouraged to state their personal reasons for and against their cannabis consumption, which they can review at any time, so they may reflect on what they could gain by successfully completing the program” [ 70 ]). Other commonly identified BCTs included social comparison (BCT 6.2; 12/19, 63% of the studies) and information about social and environmental consequences (BCT 5.3; 11/19, 58% of the studies), followed by problem solving (BCT 2.1; 10/19, 53% of the studies) and information about health consequences (BCT 5.1; 10/19, 53% of the studies).
RoB Assessment
Figure 2 presents the overall assessment of risk in each domain for all the included studies, whereas Figure 3 [ 70 - 72 , 77 - 92 ] summarizes the assessment of each study at the outcome level for each domain in the Cochrane RoB 2 [ 74 ].
Figure 2 shows that, of the included studies, 93% (27/29) were rated as having a “low” RoB arising from the randomization process (ie, selection bias) and 83% (24/29) were rated as having a “low” RoB due to missing data (ie, attrition bias). For bias due to deviations from the intended intervention (ie, performance bias), 72% (21/29) were rated as having a “low” risk, and for selective reporting of results, 59% (17/29) were rated as having a “low” risk. In the remaining domain regarding bias in measurement of the outcome (ie, detection bias), 48% (14/29) of the studies were deemed to present “some concerns,” mainly owing to the outcome assessment not being blinded (eg, self-reported outcome measure of CU). Finally, 79% (15/19) of the included studies were deemed to present “some concerns” or were rated as having a “high” RoB at the outcome level ( Figure 3 [ 70 - 72 , 77 - 92 ]). The RoB assessment for CU and cannabis consequences of each included study is presented in Multimedia Appendix 9 [ 70 - 72 , 77 - 92 ].

Meta-Analysis Results
Due to several missing data points and despite contacting the authors, we were able to carry out only 1 meta-analysis of our primary outcome, CU frequency. Usable data were retrieved from only 16% (3/19) [ 70 - 72 ] of the studies included in this review. These 3 studies provided sufficient information to calculate an effect size, including mean differences based on change-from-baseline measurements and associated 95% CIs (or SE of the mean difference) and sample sizes per intervention and comparison conditions. The reasons for excluding the other 84% (16/19) of the studies included heterogeneity in outcome variables or measurements, inconsistent results, and missing data ( Multimedia Appendix 10 [ 77 - 92 ]).
Figure 4 [ 70 - 72 ] illustrates the mean differences and associated 95% CIs of 3 unique RCTs [ 70 - 72 ] that provided sufficient information to allow for the measurement of CU frequency at 3 months after the baseline relative to a comparison condition in terms of the number of self-reported days of use in the previous month using the TLFB method. Overall, the synthesized effect of digital interventions for young adult cannabis users on CU frequency, as measured using days of use in the previous month, was −6.79 (95% CI −9.59 to −4.00). This suggests that digital CU interventions had a statistically significant effect ( P <.001) on reducing CU frequency at the 3-month follow-up compared with the control conditions (both passive and active controls). The results of the meta-analysis also showed low between-study heterogeneity ( I 2 =48.3%; P =.12) across the 3 included studies.

The samples of the 3 studies included in the meta-analysis varied in size from 225 to 1292 participants (mean 697.33, SD 444.11), and the mean age ranged from 24.7 to 31.88 years (mean 26.38, SD 3.58 years). These studies involved 3 different digital interventions and used different design approaches to assess intervention effectiveness. One study assessed the effectiveness of a web-based counseling program (ie, Quit the Shit) against a waitlist control [ 72 ], another examined the effectiveness of a fully self-guided web-based treatment program for CU and related problems (ie, Reduce Your Use: How to Break the Cannabis Habit) against a control condition website consisting of basic educational information on cannabis [ 71 ], and the third used a 3-arm RCT design to investigate whether the effectiveness of a minimally guided internet-based self-help intervention (ie, CANreduce 2.0) might be enhanced by implementing adherence-focused guidance and emphasizing the social presence factor of a personal e-coach [ 70 ].
Summary of Principal Findings
The primary aim of this systematic review was to evaluate the effectiveness of digital interventions in addressing CU among community-living young adults. We included 19 randomized controlled studies representing 9 unique digital interventions aimed at preventing, reducing, or ceasing CU and evaluated the effects of 3 different digital interventions on CU. In summary, the 3 digital interventions included in the meta-analysis proved superior to control conditions in reducing the number of days of CU in the previous month at the 3-month follow-up.
Our findings are consistent with those of 2 previous meta-analyses by Olmos et al [ 43 ] and Tait et al [ 44 ] and with the findings of a recently published umbrella review of systematic reviews and meta-analyses of RCTs [ 123 ], all of which revealed a positive effect of internet- and computer-based interventions on CU. However, a recent systematic review and meta-analysis by Beneria et al [ 45 ] found that web-based CU interventions did not significantly reduce CU. Beneria et al [ 45 ] included studies with different intervention programs that targeted diverse population groups (both adolescents and young adults) and use of more than one substance (eg, alcohol and cannabis). In our systematic review, a more conservative approach was taken—we focused specifically on young adults and considered interventions targeting CU only. Although our results indicate that digital interventions hold great promise in terms of effectiveness, an important question that remains unresolved is whether there is an optimal exposure dose in terms of both duration and frequency that might be more effective. Among the studies included in this systematic review, interventions varied considerably in terms of the number of psychoeducational modules offered (from 2 to 13), time spent reviewing the material, and duration (from a single session to a 12-week spread period). Our results suggest that an intervention duration of at least 6 weeks yields better results.
Another important finding of this review is that, although almost half (9/19, 47%) of the included studies observed an intervention effect on CU frequency, none reported a statistically significant improvement in cannabis-related negative consequences, which may be considered a more distal indicator. More than half (10/19, 53%) of the included studies investigated this outcome. It seems normal to expect to find an effect on CU frequency given that reducing CU is often the primary objective of interventions and because the motivation of users’ is generally focused on changing consumption behavior. It is plausible to think that the change in behavior at the consumption level must be maintained over time before an effect on cannabis-related negative consequences can be observed. However, our results showed that, in all the included studies, cannabis-related negative consequences and change in behavior (CU frequency) were measured at the same time point, namely, 3 months after the baseline. Moreover, Grigsby et al [ 124 ] conducted a scoping review of risk and protective factors for CU and suggested that interventions to reduce negative CU consequences should prioritize multilevel methods or strategies “to attenuate the cumulative risk from a combination of psychological, contextual, and social influences.”
A secondary objective of this systematic review was to describe the active ingredients used in digital interventions for CU among young adults. The vast majority of the interventions were based on either a theory or an intervention approach derived from theories such as CBT, MI, and personalized feedback. From these theories and approaches stem behavior change strategies or techniques, commonly known as BCTs. Feedback on behavior , included in the feedback monitoring BCT cluster, was the most common BCT used in the included studies. This specific BCT appears to be a core strategy in behavior change interventions [ 125 , 126 ]. In their systematic review of remotely delivered alcohol or substance misuse interventions for adults, Howlett et al [ 53 ] found that feedback on behavior , problem solving , and goal setting were the most frequently used BCTs in the included studies. In addition, this research group noted that the most promising BCTs for alcohol misuse were avoidance/reducing exposure to cues for behavior , pros and cons , and self-monitoring of behavior, whereas 2 very promising strategies for substance misuse in general were problem solving and self-monitoring of behavior . In our systematic review, in addition to feedback on behavior , the 6 most frequently used BCTs in the included studies were social support , pros and cons , social comparison , problem solving , information about social and environmental consequences , and information about health consequences . Although pros and cons and problem solving were present in all 3 studies of digital interventions included in our meta-analysis, avoidance/reducing exposure to cues for behavior was reported in only 5% (1/19) of the articles, and feedback on behavior was more frequently used than self-monitoring of behavior. However, it should be noted that the review by Howlett et al [ 53 ] examined digital interventions for participants with alcohol or substance misuse problems, whereas in this review, we focused on interventions that targeted CU from a harm reduction perspective. In this light, avoidance/reducing exposure to cues for behavior may be a BCT better suited to populations with substance misuse problems. Lending support to this, a meta-regression by Garnett et al [ 127 ] and a Cochrane systematic review by Kaner et al [ 128 ] both found interventions that used behavior substitution and credible source to be associated with greater reduction in excessive alcohol consumption compared with interventions that used other BCTs.
Beyond the number and types of BCTs used, reflecting on the extent to which each BCT in a given intervention suits (or does not suit) the targeted determinants (ie, behavioral and environmental causes) is crucial for planning intervention programs [ 26 ]. It is important when designing digital CU interventions not merely to pick a combination of BCTs that have been associated with effectiveness. Rather, the active ingredients must fit the determinants that the interventionists seek to influence. For example, action planning would be more relevant as a BCT for young adults highly motivated and ready to take action on their CU than would pros and cons , which aims instead to bolster motivation. Given that more than half of all digital interventions are asynchronous and based on a self-guided approach and do not offer counselor or therapist support, a great deal of motivation is required to engage in intervention and behavior change. Therefore, it is essential that developers consider the needs and characteristics of the targeted population to tailor intervention strategies (ie, BCTs) for successful behavior change (eg, tailored to the participant’s stage of change). In most of the digital interventions included in this systematic review, personalization was achieved through feedback messages about CU regarding descriptive norms, motives, risks and consequences, and costs, among other things.
Despite the high number of recent studies conducted in the field of digital CU interventions, most of the included articles in our review (17/19, 89%) reported on the development and evaluation of web-based intervention programs. A new generation of health intervention modalities such as mobile apps and social media has drawn the attention of researchers in the past decade and is currently being evaluated. In this regard, the results from a recently published scoping review [ 129 ], which included 5 studies of mobile apps for nonmedical CU, suggested that these novel modes of intervention delivery demonstrated adequate feasibility and acceptability. Nevertheless, the internet remains a powerful and convenient medium for reaching young adults with digital interventions intended to support safe CU behaviors [ 123 , 130 ].
Quality of Evidence
The GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach [ 131 - 133 ] was used to assess the quality of the evidence reviewed. It was deemed to be moderate for the primary outcome of this review, that is, CU frequency in terms of days of use in the previous month (see the summary of evidence in Multimedia Appendix 11 [ 70 , 72 ]). The direction of evidence was broadly consistent—in all 3 RCT studies [ 70 - 72 ] included in the meta-analysis, participants who received digital CU interventions reduced their consumption compared with those who received no or minimal interventions. The 3 RCTs were similar in that they all involved a web-based, multicomponent intervention program aimed at reducing or ceasing CU. However, the interventions did differ or vary in terms of several characteristics, including the strategies used, content, frequency, and duration. Given the small number of studies included in the meta-analysis, we could not conclude with certainty which intervention components, if any, contributed to the effect estimate observed.
Although inconsistency, indirectness, and imprecision were not major issues in the body of evidence, we downgraded the evidence from high to moderate quality on account of RoB assessments at the outcome level. The 3 RCT studies included in the meta-analysis were rated as having “some concerns” of RoB, mainly due to lack of blinding, which significantly reduced our certainty relative to subjective outcomes (ie, self-reported measures of CU frequency). A positive feature of these digital intervention trials is that most procedures are fully automated, and so there was typically a low RoB regarding randomization procedures, allocation to different conditions, and intervention delivery. It is impossible to blind participants to these types of behavior change interventions, and although some researchers have made attempts to counter the impact of this risk, performance bias is an inescapable issue in RCT studies of this kind. Blinding of intervention providers was not an issue in the 3 RCTs included in the meta-analysis because outcome data collection was automated. However, this same automated procedure made it very difficult to ensure follow‐up. Consequently, attrition was another source of bias in these RCT studies [ 70 - 72 ]. The participants lost to follow-up likely stopped using the intervention. However, there is no way of determining whether these people would have benefited more or less than the completers if they had seen the trial through.
The 3 RCTs included in the meta-analysis relied on subjective self-reported measures of CU at baseline and follow‐up, which are subject to recall and social desirability bias. However, all 3 studies used a well-validated instrument of measurement to determine frequency of CU, the TLFB [ 66 ]. This is a widely used, subjective self-report tool for measuring frequency (or quantity) of substance use (or abstinence). It is considered a reliable measure of CU [ 134 , 135 ]. Finally, it should be pointed out that any potential bias related to self‐reported CU frequency would have affected both the intervention and control groups (particularly in cases in which control groups received cannabis‐related information), and thus, it was unlikely to account for differential intervention effects. Moreover, we found RoB due to selective reporting in some studies owing mainly to the absence of any reference to a protocol. Ultimately, these limitations may have biased the results of the meta-analysis. Consequently, future research is likely to further undermine our confidence in the effect estimate we observed and report considerably different estimates.
Strengths and Limitations
Our systematic review and meta-analysis has a number of strengths: (1) we included only randomized controlled studies to ensure that the included studies possessed a rigorous research design, (2) we focused specifically on cannabis (rather than combining multiple substances), (3) we assessed the effectiveness of 3 different digital interventions on CU frequency among community-living young adults, and (4) we performed an exhaustive synthesis and comparison of the BCTs used in the 9 digital interventions examined in the 19 studies included in our review based on the BCTTv1.
Admittedly, this systematic review and meta-analysis has limitations that should be recognized. First, although we searched a range of bibliographic databases, the review was limited to articles published in peer-reviewed journals in English or French. This may have introduced publication bias given that articles reporting positive effects are more likely to be published than those with negative or equivocal results. Consequently, the studies included in this review may have overrepresented the statistically significant effects of digital CU interventions.
Second, only a small number of studies were included in the meta-analyses because many studies did not provide adequate statistical information for calculating and synthesizing effect sizes, although significant efforts were made to contact the authors in case of missing data. Because of the small sample size used in the meta-analysis, the effect size estimates may not be highly reflective of the true effects of digital interventions on CU frequency among young adults. Furthermore, synthesizing findings across studies that evaluated different modalities of web-based intervention programs (eg, fully self-guided vs with therapist guidance) and types of intervention approaches (eg, CBT, MI, and personalized feedback) may have introduced bias in the meta-analytical results due to the heterogeneity of the included studies, although heterogeneity was controlled for using a random-effects model and our results indicated low between-study heterogeneity.
Third, we took various measures to ensure that BCT coding was carried out rigorously throughout the data extraction and analysis procedures: (1) all coders received training on how to use the BCTTv1; (2) all the included articles were read line by line so that coders became familiar with intervention descriptions before initiating BCT coding; (3) the intervention description of each included article was double coded after a pilot calibration exercise with all coders, and any disagreements regarding the presence or absence of a BCT were discussed and resolved with a third party; and (4) we contacted the article authors when necessary and possible for further details on the BCTs they used. However, incomplete reporting of intervention content is a recognized issue [ 136 ], which may have resulted in our coding BCTs incorrectly as present or absent. Reliably specifying the BCTs used in interventions allows their active ingredients to be identified, their evidence to be synthesized, and interventions to be replicated, thereby providing tangible guidance to programmers and researchers to develop more effective interventions.
Finally, although this review identified the BCTs used in digital interventions, our approach did not allow us to draw conclusions regarding their effectiveness. Coding BCTs simply as present or absent does not consider the frequency, intensity, and quality with which they were delivered. For example, it is unclear how many individuals should self‐monitor their CU. In addition, the quality of BCT implementation may be critical in digital interventions where different graphics and interface designs and the usability of the BCTs used can have considerable influence on the level of user engagement [ 137 ]. In the future, it may be necessary to develop new methods to evaluate the dosage of individual BCTs in digital health interventions and characterize their implementation quality to assess their effectiveness [ 128 , 138 ]. Despite its limitations, this review suggests that digital interventions represent a promising avenue for preventing, reducing, or ceasing CU among community-living young adults.
Conclusions
The results of this systematic review and meta-analysis lend support to the promise of digital interventions as an effective means of reducing recreational CU frequency among young adults. Despite the advent and popularity of smartphones, web-based interventions remain the most common mode of delivery for digital interventions. The active ingredients of digital interventions are varied and encompass a number of clusters of the BCTTv1, but a significant number of BCTs remain underused. Additional research is needed to further investigate the effectiveness of these interventions on CU and key outcomes at later time points. Finally, a detailed assessment of user engagement with digital interventions for CU and understanding which intervention components are the most effective remain important research gaps.
Acknowledgments
The authors would like to thank Bénédicte Nauche, Miguel Chagnon, and Paul Di Biase for their valuable support with the search strategy development, statistical analysis, and linguistic revision, respectively. This work was supported by the Ministère de la Santé et des Services sociaux du Québec as part of a broader study aimed at developing and evaluating a digital intervention for young adult cannabis users. Additional funding was provided by the Research Chair in Innovative Nursing Practices. The views and opinions expressed in this manuscript do not necessarily reflect those of these funding entities.
Data Availability
The data sets generated and analyzed during this study are available from the corresponding author on reasonable request.
Authors' Contributions
JC contributed to conceptualization, methodology, formal analysis, writing—original draft, supervision, and funding acquisition. GC contributed to conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, visualization, and project administration. BV contributed to conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, and visualization. PA contributed to conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, visualization, and project administration. GR contributed to conceptualization, methodology, formal analysis, investigation, data curation, and writing—review and editing. GF contributed to conceptualization, methodology, formal analysis, investigation, data curation, and writing—review and editing. DJA contributed to conceptualization, methodology, formal analysis, writing—review and editing, and funding acquisition.
Conflicts of Interest
None declared.
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Detailed search strategies for each database.
Population, intervention, comparison, outcome, and study design strategy.
Excluded studies and reasons for exclusion.
Study and participant characteristics.
Description of intervention characteristics in the included articles.
Summary of methodological characteristics and major findings of the included studies categorized by intervention name.
Behavior change techniques (BCTs) coded in each included study summarized by individual BCT and BCT cluster.
Risk-of-bias assessment of each included study for cannabis use and cannabis consequences.
Excluded studies and reasons for exclusion from the meta-analysis.
Summary of evidence according to the Grading of Recommendations Assessment, Development, and Evaluation tool.
- Arnett JJ. The developmental context of substance use in emerging adulthood. J Drug Issues. 2005;35(2):235-254. [ CrossRef ]
- Stockings E, Hall WD, Lynskey M, Morley KI, Reavley N, Strang J, et al. Prevention, early intervention, harm reduction, and treatment of substance use in young people. Lancet Psychiatry. Mar 2016;3(3):280-296. [ CrossRef ] [ Medline ]
- ElSohly MA, Chandra S, Radwan M, Majumdar CG, Church JC. A comprehensive review of cannabis potency in the United States in the last decade. Biol Psychiatry Cogn Neurosci Neuroimaging. Jun 2021;6(6):603-606. [ CrossRef ] [ Medline ]
- Fischer B, Robinson T, Bullen C, Curran V, Jutras-Aswad D, Medina-Mora ME, et al. Lower-Risk Cannabis Use Guidelines (LRCUG) for reducing health harms from non-medical cannabis use: a comprehensive evidence and recommendations update. Int J Drug Policy. Jan 2022;99:103381. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Rotermann M. What has changed since cannabis was legalized? Health Rep. Feb 19, 2020;31(2):11-20. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Degenhardt L, Stockings E, Patton G, Hall WD, Lynskey M. The increasing global health priority of substance use in young people. Lancet Psychiatry. Mar 2016;3(3):251-264. [ CrossRef ] [ Medline ]
- Buckner JD, Bonn-Miller MO, Zvolensky MJ, Schmidt NB. Marijuana use motives and social anxiety among marijuana-using young adults. Addict Behav. Oct 2007;32(10):2238-2252. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Carliner H, Brown QL, Sarvet AL, Hasin DS. Cannabis use, attitudes, and legal status in the U.S.: a review. Prev Med. Nov 2017;104:13-23. [ FREE Full text ] [ CrossRef ] [ Medline ]
- World drug report 2020. United Nations Office on Drugs and Crime. 2020. URL: https://wdr.unodc.org/wdr2020/index2020.html [accessed 2023-11-28]
- National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division, Board on Population Health and Public Health Practice, Committee on the Health Effects of Marijuana: An Evidence Review and Research Agenda. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC. The National Academies Press; 2017.
- Hall WD, Patton G, Stockings E, Weier M, Lynskey M, Morley KI, et al. Why young people's substance use matters for global health. Lancet Psychiatry. Mar 2016;3(3):265-279. [ CrossRef ] [ Medline ]
- Cohen K, Weizman A, Weinstein A. Positive and negative effects of cannabis and cannabinoids on health. Clin Pharmacol Ther. May 2019;105(5):1139-1147. [ CrossRef ] [ Medline ]
- Memedovich KA, Dowsett LE, Spackman E, Noseworthy T, Clement F. The adverse health effects and harms related to marijuana use: an overview review. CMAJ Open. Aug 16, 2018;6(3):E339-E346. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Teeters JB, Armstrong NM, King SA, Hubbard SM. A randomized pilot trial of a mobile phone-based brief intervention with personalized feedback and interactive text messaging to reduce driving after cannabis use and riding with a cannabis impaired driver. J Subst Abuse Treat. Nov 2022;142:108867. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Chan GC, Becker D, Butterworth P, Hines L, Coffey C, Hall W, et al. Young-adult compared to adolescent onset of regular cannabis use: a 20-year prospective cohort study of later consequences. Drug Alcohol Rev. May 2021;40(4):627-636. [ CrossRef ] [ Medline ]
- Hall W, Stjepanović D, Caulkins J, Lynskey M, Leung J, Campbell G, et al. Public health implications of legalising the production and sale of cannabis for medicinal and recreational use. Lancet. Oct 26, 2019;394(10208):1580-1590. [ CrossRef ] [ Medline ]
- The health and social effects of nonmedical cannabis use. World Health Organization. 2016. URL: https://apps.who.int/iris/handle/10665/251056 [accessed 2023-11-28]
- Boumparis N, Loheide-Niesmann L, Blankers M, Ebert DD, Korf D, Schaub MP, et al. Short- and long-term effects of digital prevention and treatment interventions for cannabis use reduction: a systematic review and meta-analysis. Drug Alcohol Depend. Jul 01, 2019;200:82-94. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Jutras-Aswad D, Le Foll B, Bruneau J, Wild TC, Wood E, Fischer B. Thinking beyond legalization: the case for expanding evidence-based options for cannabis use disorder treatment in Canada. Can J Psychiatry. Feb 2019;64(2):82-87. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Garnett CV, Crane D, Brown J, Kaner EF, Beyer FR, Muirhead CR, et al. Behavior change techniques used in digital behavior change interventions to reduce excessive alcohol consumption: a meta-regression. Ann Behav Med. May 18, 2018;52(6):530-543. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Glanz K, Rimer BK, Viswanath K. Health Behavior: Theory, Research, and Practice, 5th Edition. Hoboken, NJ. Jossey-Bass; Jul 2015.
- Prestwich A, Webb TL, Conner M. Using theory to develop and test interventions to promote changes in health behaviour: evidence, issues, and recommendations. Curr Opin Psychol. Oct 2015;5:1-5. [ CrossRef ]
- Webb TL, Sniehotta FF, Michie S. Using theories of behaviour change to inform interventions for addictive behaviours. Addiction. Nov 2010;105(11):1879-1892. [ CrossRef ] [ Medline ]
- Cilliers F, Schuwirth L, van der Vleuten C. Health behaviour theories: a conceptual lens to explore behaviour change. In: Cleland J, Durning SJ, editors. Researching Medical Education. Hoboken, NJ. Wiley; 2015.
- Davis R, Campbell R, Hildon Z, Hobbs L, Michie S. Theories of behaviour and behaviour change across the social and behavioural sciences: a scoping review. Health Psychol Rev. 2015;9(3):323-344. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Eldredge LK, Markham CM, Ruiter RA, Fernández ME, Kok G, Parcel GS. Planning Health Promotion Programs: An Intervention Mapping Approach, 4th Edition. Hoboken, NJ. John Wiley & Sons; Feb 2016.
- Marlatt GA, Blume AW, Parks GA. Integrating harm reduction therapy and traditional substance abuse treatment. J Psychoactive Drugs. 2001;33(1):13-21. [ CrossRef ] [ Medline ]
- Adams A, Ferguson M, Greer AM, Burmeister C, Lock K, McDougall J, et al. Guideline development in harm reduction: considerations around the meaningful involvement of people who access services. Drug Alcohol Depend Rep. Aug 12, 2022;4:100086. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Davis ML, Powers MB, Handelsman P, Medina JL, Zvolensky M, Smits JA. Behavioral therapies for treatment-seeking cannabis users: a meta-analysis of randomized controlled trials. Eval Health Prof. Mar 2015;38(1):94-114. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Gates PJ, Sabioni P, Copeland J, Le Foll B, Gowing L. Psychosocial interventions for cannabis use disorder. Cochrane Database Syst Rev. May 05, 2016;2016(5):CD005336. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Halladay J, Scherer J, MacKillop J, Woock R, Petker T, Linton V, et al. Brief interventions for cannabis use in emerging adults: a systematic review, meta-analysis, and evidence map. Drug Alcohol Depend. Nov 01, 2019;204:107565. [ CrossRef ] [ Medline ]
- Imtiaz S, Roerecke M, Kurdyak P, Samokhvalov AV, Hasan OS, Rehm J. Brief interventions for cannabis use in healthcare settings: systematic review and meta-analyses of randomized trials. J Addict Med. 2020;14(1):78-88. [ CrossRef ] [ Medline ]
- Standeven LR, Scialli A, Chisolm MS, Terplan M. Trends in cannabis treatment admissions in adolescents/young adults: analysis of TEDS-A 1992 to 2016. J Addict Med. 2020;14(4):e29-e36. [ CrossRef ] [ Medline ]
- Montanari L, Guarita B, Mounteney J, Zipfel N, Simon R. Cannabis use among people entering drug treatment in europe: a growing phenomenon? Eur Addict Res. 2017;23(3):113-121. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Kerridge BT, Mauro PM, Chou SP, Saha TD, Pickering RP, Fan AZ, et al. Predictors of treatment utilization and barriers to treatment utilization among individuals with lifetime cannabis use disorder in the United States. Drug Alcohol Depend. Dec 01, 2017;181:223-228. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Gates P, Copeland J, Swift W, Martin G. Barriers and facilitators to cannabis treatment. Drug Alcohol Rev. May 2012;31(3):311-319. [ CrossRef ] [ Medline ]
- Hammarlund RA, Crapanzano KA, Luce L, Mulligan L, Ward KM. Review of the effects of self-stigma and perceived social stigma on the treatment-seeking decisions of individuals with drug- and alcohol-use disorders. Subst Abuse Rehabil. Nov 23, 2018;9:115-136. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Bedrouni W. On the use of digital technologies to reduce the public health impacts of cannabis legalization in Canada. Can J Public Health. Dec 2018;109(5-6):748-751. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Perski O, Hébert ET, Naughton F, Hekler EB, Brown J, Businelle MS. Technology-mediated just-in-time adaptive interventions (JITAIs) to reduce harmful substance use: a systematic review. Addiction. May 2022;117(5):1220-1241. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Kazemi DM, Borsari B, Levine MJ, Li S, Lamberson KA, Matta LA. A systematic review of the mHealth interventions to prevent alcohol and substance abuse. J Health Commun. May 2017;22(5):413-432. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Nesvåg S, McKay JR. Feasibility and effects of digital interventions to support people in recovery from substance use disorders: systematic review. J Med Internet Res. Aug 23, 2018;20(8):e255. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Hoch E, Preuss UW, Ferri M, Simon R. Digital interventions for problematic cannabis users in non-clinical settings: findings from a systematic review and meta-analysis. Eur Addict Res. 2016;22(5):233-242. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Olmos A, Tirado-Muñoz J, Farré M, Torrens M. The efficacy of computerized interventions to reduce cannabis use: a systematic review and meta-analysis. Addict Behav. Apr 2018;79:52-60. [ CrossRef ] [ Medline ]
- Tait RJ, Spijkerman R, Riper H. Internet and computer based interventions for cannabis use: a meta-analysis. Drug Alcohol Depend. Dec 01, 2013;133(2):295-304. [ CrossRef ] [ Medline ]
- Beneria A, Santesteban-Echarri O, Daigre C, Tremain H, Ramos-Quiroga JA, McGorry PD, et al. Online interventions for cannabis use among adolescents and young adults: systematic review and meta-analysis. Early Interv Psychiatry. Aug 2022;16(8):821-844. [ CrossRef ] [ Medline ]
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. Int J Nurs Stud. May 2013;50(5):587-592. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Michie S, Abraham C, Eccles MP, Francis JJ, Hardeman W, Johnston M. Strengthening evaluation and implementation by specifying components of behaviour change interventions: a study protocol. Implement Sci. Feb 07, 2011;6:10. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. Aug 2013;46(1):81-95. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Michie S, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: mapping theoretically derived behavioural determinants to behaviour change techniques. Appl Psychol. Oct 2008;57(4):660-680. [ CrossRef ]
- Scott C, de Barra M, Johnston M, de Bruin M, Scott N, Matheson C, et al. Using the behaviour change technique taxonomy v1 (BCTTv1) to identify the active ingredients of pharmacist interventions to improve non-hospitalised patient health outcomes. BMJ Open. Sep 15, 2020;10(9):e036500. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Dombrowski SU, Sniehotta FF, Avenell A, Johnston M, MacLennan G, Araújo-Soares V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: a systematic review. Health Psychol Rev. 2012;6(1):7-32. [ CrossRef ]
- Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. Nov 2009;28(6):690-701. [ CrossRef ] [ Medline ]
- Howlett N, García-Iglesias J, Bontoft C, Breslin G, Bartington S, Freethy I, et al. A systematic review and behaviour change technique analysis of remotely delivered alcohol and/or substance misuse interventions for adults. Drug Alcohol Depend. Oct 01, 2022;239:109597. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions Version 6.4. London, UK. The Cochrane Collaboration; 2023.
- Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. Mar 29, 2021;372:n160. [ FREE Full text ] [ CrossRef ] [ Medline ]
- McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. Jul 2016;75:40-46. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Halladay J, Petker T, Fein A, Munn C, MacKillop J. Brief interventions for cannabis use in emerging adults: protocol for a systematic review, meta-analysis, and evidence map. Syst Rev. Jul 25, 2018;7(1):106. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. Apr 23, 2011;6:42. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. Am Psychol. May 2000;55(5):469-480. [ Medline ]
- Bramer WM, Giustini D, de Jonge GB, Holland L, Bekhuis T. De-duplication of database search results for systematic reviews in EndNote. J Med Libr Assoc. Jul 2016;104(3):240-243. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. Mar 07, 2014;348:g1687. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Presseau J, Ivers NM, Newham JJ, Knittle K, Danko KJ, Grimshaw JM. Using a behaviour change techniques taxonomy to identify active ingredients within trials of implementation interventions for diabetes care. Implement Sci. Apr 23, 2015;10:55. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Fontaine G, Cossette S, Maheu-Cadotte MA, Deschênes MF, Rouleau G, Lavallée A, et al. Effect of implementation interventions on nurses' behaviour in clinical practice: a systematic review, meta-analysis and meta-regression protocol. Syst Rev. Dec 05, 2019;8(1):305. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Fontaine G, Cossette S. A theory-based adaptive E-learning program aimed at increasing intentions to provide brief behavior change counseling: randomized controlled trial. Nurse Educ Today. Dec 2021;107:105112. [ CrossRef ] [ Medline ]
- Fontaine G, Cossette S. Development and design of E_MOTIV: a theory-based adaptive e-learning program to support nurses' provision of brief behavior change counseling. Comput Inform Nurs. Mar 01, 2023;41(3):130-141. [ CrossRef ] [ Medline ]
- Sobell LC, Sobell MB. Timeline follow-back: a technique for assessing self-reported alcohol consumption. In: Litten RZ, Allen JP, editors. Measuring Alcohol Consumption. Totowa, NJ. Humana Press; 1992.
- Stephens RS, Roffman RA, Simpson EE. Treating adult marijuana dependence: a test of the relapse prevention model. J Consult Clin Psychol. 1994;62(1):92-99. [ CrossRef ]
- Harris RJ, Deeks JJ, Altman DG, Bradburn MJ, Harbord RM, Sterne JA. Metan: fixed- and random-effects meta-analysis. Stata J. 2008;8(1):3-28. [ CrossRef ]
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. Sep 06, 2003;327(7414):557-560. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Baumgartner C, Schaub MP, Wenger A, Malischnig D, Augsburger M, Walter M, et al. CANreduce 2.0 adherence-focused guidance for internet self-help among cannabis users: three-arm randomized controlled trial. J Med Internet Res. Apr 30, 2021;23(4):e27463. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Rooke S, Copeland J, Norberg M, Hine D, McCambridge J. Effectiveness of a self-guided web-based cannabis treatment program: randomized controlled trial. J Med Internet Res. Feb 15, 2013;15(2):e26. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Tossmann HP, Jonas B, Tensil MD, Lang P, Strüber E. A controlled trial of an internet-based intervention program for cannabis users. Cyberpsychol Behav Soc Netw. Nov 2011;14(11):673-679. [ CrossRef ] [ Medline ]
- StataCorp. Stata statistical software: release 18. StataCorp LLC. College Station, TX. StataCorp LLC; 2023. URL: https://www.stata.com/ [accessed 2023-11-28]
- Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. Aug 28, 2019;366:l4898. [ FREE Full text ] [ CrossRef ] [ Medline ]
- McGuinness LA, Higgins JP. Risk-of-bias VISualization (robvis): an R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods. Jan 2021;12(1):55-61. [ CrossRef ] [ Medline ]
- Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: an R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and open synthesis. Campbell Syst Rev. Mar 27, 2022;18(2):e1230. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Elliott JC, Carey KB. Correcting exaggerated marijuana use norms among college abstainers: a preliminary test of a preventive intervention. J Stud Alcohol Drugs. Nov 2012;73(6):976-980. [ CrossRef ] [ Medline ]
- Elliott JC, Carey KB, Vanable PA. A preliminary evaluation of a web-based intervention for college marijuana use. Psychol Addict Behav. Mar 2014;28(1):288-293. [ CrossRef ] [ Medline ]
- Lee CM, Neighbors C, Kilmer JR, Larimer ME. A brief, web-based personalized feedback selective intervention for college student marijuana use: a randomized clinical trial. Psychol Addict Behav. Jun 2010;24(2):265-273. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Buckner JD, Zvolensky MJ, Lewis EM. On-line personalized feedback intervention for negative affect and cannabis: a pilot randomized controlled trial. Exp Clin Psychopharmacol. Apr 2020;28(2):143-149. [ CrossRef ] [ Medline ]
- Goodness TM, Palfai TP. Electronic screening and brief intervention to reduce cannabis use and consequences among graduate students presenting to a student health center: a pilot study. Addict Behav. Jul 2020;106:106362. [ CrossRef ] [ Medline ]
- Palfai TP, Saitz R, Winter M, Brown TA, Kypri K, Goodness TM, et al. Web-based screening and brief intervention for student marijuana use in a university health center: pilot study to examine the implementation of eCHECKUP TO GO in different contexts. Addict Behav. Sep 2014;39(9):1346-1352. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Riggs NR, Conner BT, Parnes JE, Prince MA, Shillington AM, George MW. Marijuana eCHECKUPTO GO: effects of a personalized feedback plus protective behavioral strategies intervention for heavy marijuana-using college students. Drug Alcohol Depend. Sep 01, 2018;190:13-19. [ CrossRef ] [ Medline ]
- Bonar EE, Chapman L, Pagoto S, Tan CY, Duval ER, McAfee J, et al. Social media interventions addressing physical activity among emerging adults who use cannabis: a pilot trial of feasibility and acceptability. Drug Alcohol Depend. Jan 01, 2023;242:109693. [ CrossRef ] [ Medline ]
- Bonar EE, Goldstick JE, Chapman L, Bauermeister JA, Young SD, McAfee J, et al. A social media intervention for cannabis use among emerging adults: randomized controlled trial. Drug Alcohol Depend. Mar 01, 2022;232:109345. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Walukevich-Dienst K, Neighbors C, Buckner JD. Online personalized feedback intervention for cannabis-using college students reduces cannabis-related problems among women. Addict Behav. Nov 2019;98:106040. [ CrossRef ] [ Medline ]
- Côté J, Tessier S, Gagnon H, April N, Rouleau G, Chagnon M. Efficacy of a web-based tailored intervention to reduce cannabis use among young people attending adult education centers in Quebec. Telemed J E Health. Nov 2018;24(11):853-860. [ CrossRef ] [ Medline ]
- Cunningham JA, Schell C, Bertholet N, Wardell JD, Quilty LC, Agic B, et al. Online personalized feedback intervention to reduce risky cannabis use. Randomized controlled trial. Internet Interv. Nov 14, 2021;26:100484. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Copeland J, Rooke S, Rodriquez D, Norberg MM, Gibson L. Comparison of brief versus extended personalised feedback in an online intervention for cannabis users: short-term findings of a randomised trial. J Subst Abuse Treat. May 2017;76:43-48. [ CrossRef ] [ Medline ]
- Jonas B, Tensil MD, Tossmann P, Strüber E. Effects of treatment length and chat-based counseling in a web-based intervention for cannabis users: randomized factorial trial. J Med Internet Res. May 08, 2018;20(5):e166. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Schaub MP, Wenger A, Berg O, Beck T, Stark L, Buehler E, et al. A web-based self-help intervention with and without chat counseling to reduce cannabis use in problematic cannabis users: three-arm randomized controlled trial. J Med Internet Res. Oct 13, 2015;17(10):e232. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Sinadinovic K, Johansson M, Johansson AS, Lundqvist T, Lindner P, Hermansson U. Guided web-based treatment program for reducing cannabis use: a randomized controlled trial. Addict Sci Clin Pract. Feb 18, 2020;15(1):9. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Kanfer FH. Implications of a self-regulation model of therapy for treatment of addictive behaviors. In: Miller WR, Heather N, editors. Treating Addictive Behaviors. Boston, MA. Springer; 1986;29-47.
- Mohr DC, Cuijpers P, Lehman K. Supportive accountability: a model for providing human support to enhance adherence to eHealth interventions. J Med Internet Res. Mar 10, 2011;13(1):e30. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Marlatt GA, Baer JS, Kivlahan DR, Dimeff LA, Larimer ME, Quigley LA, et al. Screening and brief intervention for high-risk college student drinkers: results from a 2-year follow-up assessment. J Consult Clin Psychol. Aug 1998;66(4):604-615. [ CrossRef ]
- Miller WR, Rollnick S. Motivational Interviewing: Preparing People for Change. New York, NY. Guilford Press; 2002.
- Prince MA, Carey KB, Maisto SA. Protective behavioral strategies for reducing alcohol involvement: a review of the methodological issues. Addict Behav. Jul 2013;38(7):2343-2351. [ CrossRef ] [ Medline ]
- Lundqvist TN. Cognitive Dysfunctions in Chronic Cannabis Users Observed During Treatment: An Integrative Approach. Stockholm, Sweden. Almqvist & Wiksell; 1997.
- Kanter JW, Puspitasari AJ, Santos MM, Nagy GA. Behavioural activation: history, evidence and promise. Br J Psychiatry. May 2012;200(5):361-363. [ CrossRef ] [ Medline ]
- Jaffee WB, D'Zurilla TJ. Personality, problem solving, and adolescent substance use. Behav Ther. Mar 2009;40(1):93-101. [ CrossRef ] [ Medline ]
- Miller W, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behavior. New York, NY. The Guilford Press; 1991.
- Gordon JR, Marlatt GA. Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors. 2nd edition. New York, NY. The Guilford Press; 2005.
- Platt JJ, Husband SD. An overview of problem-solving and social skills approaches in substance abuse treatment. Psychotherapy (Chic). 1993;30(2):276-283. [ FREE Full text ]
- Steinberg KL, Roffman R, Carroll K, McRee B, Babor T, Miller M. Brief counseling for marijuana dependence: a manual for treating adults. Center for Substance Abuse Treatment, Substance Abuse and Mental Health Services Administration, US Department of Health and Human Services. URL: https://store.samhsa.gov/product/brief-counseling-marijuana-dependence-manual-treating-adults/sma15-4211 [accessed 2024-03-23]
- de Shazer S, Dolan Y. More Than Miracles: The State of the Art of Solution-Focused Brief Therapy. Oxfordshire, UK. Routledge; 2007.
- Copeland J, Swift W, Roffman R, Stephens R. A randomized controlled trial of brief cognitive-behavioral interventions for cannabis use disorder. J Subst Abuse Treat. Sep 2001;21(2):55-65. [ CrossRef ] [ Medline ]
- Linke S, McCambridge J, Khadjesari Z, Wallace P, Murray E. Development of a psychologically enhanced interactive online intervention for hazardous drinking. Alcohol Alcohol. 2008;43(6):669-674. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Wang ML, Waring ME, Jake-Schoffman DE, Oleski JL, Michaels Z, Goetz JM, et al. Clinic versus online social network-delivered lifestyle interventions: protocol for the get social noninferiority randomized controlled trial. JMIR Res Protoc. Dec 11, 2017;6(12):e243. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Sepah SC, Jiang L, Peters AL. Translating the diabetes prevention program into an online social network: validation against CDC standards. Diabetes Educ. Jul 2014;40(4):435-443. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Cunningham JA, van Mierlo T. The check your cannabis screener: a new online personalized feedback tool. Open Med Inform J. May 07, 2009;3:27-31. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Bertholet N, Cunningham JA, Faouzi M, Gaume J, Gmel G, Burnand B, et al. Internet-based brief intervention for young men with unhealthy alcohol use: a randomized controlled trial in a general population sample. Addiction. Nov 2015;110(11):1735-1743. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Walker DD, Roffman RA, Stephens RS, Wakana K, Berghuis J, Kim W. Motivational enhancement therapy for adolescent marijuana users: a preliminary randomized controlled trial. J Consult Clin Psychol. Jun 2006;74(3):628-632. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Miller MB, Leffingwell T, Claborn K, Meier E, Walters S, Neighbors C. Personalized feedback interventions for college alcohol misuse: an update of Walters and Neighbors (2005). Psychol Addict Behav. Dec 2013;27(4):909-920. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Ajzen I. From intentions to actions: a theory of planned behavior. In: Kuhl J, Beckmann J, editors. Action Control. Berlin, Germany. Springer; 1985;11-39.
- Dennis M, Titus JC, Diamond G, Donaldson J, Godley SH, Tims FM, et al. The Cannabis Youth Treatment (CYT) experiment: rationale, study design and analysis plans. Addiction. Dec 11, 2002;97 Suppl 1(s1):16-34. [ CrossRef ] [ Medline ]
- Simons JS, Dvorak RD, Merrill JE, Read JP. Dimensions and severity of marijuana consequences: development and validation of the Marijuana Consequences Questionnaire (MACQ). Addict Behav. May 2012;37(5):613-621. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Legleye S. The Cannabis Abuse Screening Test and the DSM-5 in the general population: optimal thresholds and underlying common structure using multiple factor analysis. Int J Methods Psychiatr Res. Jun 10, 2018;27(2):e1597. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Legleye S, Karila LM, Beck F, Reynaud M. Validation of the CAST, a general population Cannabis Abuse Screening Test. J Subst Use. Jul 12, 2009;12(4):233-242. [ CrossRef ]
- Sobell LC, Sobell MB. Timeline follow back. In: Litten RZ, Allen JP, editors. Measuring Alcohol Consumption: Psychosocial and Biochemical Methods. Totowa, NJ. Humana Press; 1992;41-72.
- White HR, Labouvie EW, Papadaratsakis V. Changes in substance use during the transition to adulthood: a comparison of college students and their noncollege age peers. J Drug Issues. Aug 03, 2016;35(2):281-306. [ CrossRef ]
- White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. J Stud Alcohol. Jan 1989;50(1):30-37. [ CrossRef ] [ Medline ]
- Cloutier RM, Natesan Batley P, Kearns NT, Knapp AA. A psychometric evaluation of the Marijuana Problems Index among college students: confirmatory factor analysis and measurement invariance by gender. Exp Clin Psychopharmacol. Dec 2022;30(6):907-917. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Guo H, Yang H, Yuan G, Zhu Z, Zhang K, Zhang X, et al. Effectiveness of information and communication technology (ICT) for addictive behaviors: an umbrella review of systematic reviews and meta-analysis of randomized controlled trials. Comput Hum Behav. Oct 2023;147:107843. [ CrossRef ]
- Grigsby TJ, Lopez A, Albers L, Rogers CJ, Forster M. A scoping review of risk and protective factors for negative cannabis use consequences. Subst Abuse. Apr 07, 2023;17:11782218231166622. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Harkin B, Webb TL, Chang BP, Prestwich A, Conner M, Kellar I, et al. Does monitoring goal progress promote goal attainment? A meta-analysis of the experimental evidence. Psychol Bull. Feb 2016;142(2):198-229. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Samdal GB, Eide GE, Barth T, Williams G, Meland E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int J Behav Nutr Phys Act. Mar 28, 2017;14(1):42. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Garnett C, Crane D, Brown J, Kaner E, Beyer F, Muirhead C. Behavior Change Techniques Used in Digital Behavior Change Interventions to Reduce Excessive Alcohol Consumption: A Meta-regression. Ann Behav Med May 18. 2018;52(6):A. [ CrossRef ]
- Kaner EF, Beyer FR, Muirhead C, Campbell F, Pienaar ED, Bertholet N, et al. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst Rev. Feb 24, 2018;2(2):CD004148. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Sedrati H, Belrhiti Z, Nejjari C, Ghazal H. Evaluation of mobile health apps for non-medical cannabis use: a scoping review. Procedia Comput Sci. 2022;196:581-589. [ CrossRef ]
- Curtis BL, Ashford RD, Magnuson KI, Ryan-Pettes SR. Comparison of smartphone ownership, social media use, and willingness to use digital interventions between generation Z and millennials in the treatment of substance use: cross-sectional questionnaire study. J Med Internet Res. Apr 17, 2019;21(4):e13050. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Schünemann H, Brożek J, Guyatt G, Oxman A. The GRADE Handbook. London, UK. The Cochrane Collaboration; 2013.
- Guyatt GH, Oxman AD, Schünemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. Apr 2011;64(4):380-382. [ CrossRef ] [ Medline ]
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. Apr 26, 2008;336(7650):924-926. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Hjorthøj CR, Hjorthøj AR, Nordentoft M. Validity of Timeline Follow-Back for self-reported use of cannabis and other illicit substances--systematic review and meta-analysis. Addict Behav. Mar 2012;37(3):225-233. [ CrossRef ] [ Medline ]
- Robinson SM, Sobell LC, Sobell MB, Leo GI. Reliability of the Timeline Followback for cocaine, cannabis, and cigarette use. Psychol Addict Behav. Mar 2014;28(1):154-162. [ CrossRef ] [ Medline ]
- Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol. May 2008;27(3):379-387. [ CrossRef ] [ Medline ]
- Garrett JJ. The Elements of User Experience: User-Centered Design for the Web and Beyond. London, UK. Pearson Education; 2010.
- Lorencatto F, West R, Bruguera C, Brose LS, Michie S. Assessing the quality of goal setting in behavioural support for smoking cessation and its association with outcomes. Ann Behav Med. Apr 24, 2016;50(2):310-318. [ FREE Full text ] [ CrossRef ] [ Medline ]
Abbreviations
Edited by T Leung, G Eysenbach; submitted 30.11.23; peer-reviewed by H Sedrati; comments to author 02.01.24; revised version received 09.01.24; accepted 08.03.24; published 17.04.24.
©José Côté, Gabrielle Chicoine, Billy Vinette, Patricia Auger, Geneviève Rouleau, Guillaume Fontaine, Didier Jutras-Aswad. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 17.04.2024.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research, is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.
- Login To RMS System
- About JETIR URP
- About All Approval and Licence
- Conference/Special Issue Proposal
- Book and Dissertation/Thesis Publication
- How start New Journal & Software
- Best Papers Award
- Mission and Vision
- Reviewer Board
- Join JETIR URP
- Call For Paper
- Research Areas
- Publication Guidelines
- Sample Paper Format
- Submit Paper Online
- Processing Charges
- Hard Copy and DOI Charges
- Check Your Paper Status
- Current Issue
- Past Issues
- Special Issues
- Conference Proposal
- Recent Conference
- Published Thesis
Contact Us Click Here
Whatsapp contact click here, published in:.
Volume 11 Issue 4 April-2024 eISSN: 2349-5162
UGC and ISSN approved 7.95 impact factor UGC Approved Journal no 63975
Unique identifier.
Published Paper ID: JETIR2404480
Registration ID: 536699
Page Number
Post-publication.
- Downlaod eCertificate, Confirmation Letter
- editor board member
- JETIR front page
- Journal Back Page
- UGC Approval 14 June W.e.f of CARE List UGC Approved Journal no 63975
Share This Article
Important links:.
- Call for Paper
- Submit Manuscript online

- AISHATU USMAN
- SHAMSU IBRAHIM
- HAMISU DODO
Cite This Article
2349-5162 | Impact Factor 7.95 Calculate by Google Scholar An International Scholarly Open Access Journal, Peer-Reviewed, Refereed Journal Impact Factor 7.95 Calculate by Google Scholar and Semantic Scholar | AI-Powered Research Tool, Multidisciplinary, Monthly, Multilanguage Journal Indexing in All Major Database & Metadata, Citation Generator
Publication Details
Download paper / preview article.
Download Paper
Preview this article, download pdf, print this page.
Impact Factor:
Impact factor calculation click here current call for paper, call for paper cilck here for more info important links:.
- Follow Us on
- Developed by JETIR
School bus driver had preliminary BAC of .133 while waiting to pick up students, police say
GREENUP COUNTY, Ky. ( WSAZ /Gray News) – A school bus driver in Kentucky was charged Tuesday with public intoxication while she was waiting to take students home.
According to a citation issued by the Flatwoods Police Department, Lisa Nichols, 57, was waiting for Greenup County students at an event.
A staff member alerted police, and Nichols admitted to drinking during dinner at a local restaurant.
Officers said the bus driver failed a preliminary breath test with results of .133 and showed signs of being intoxicated.
Flatwoods Police charged Nichols with alcohol intoxication in a public place.

According to Greenup County Schools Superintendent Traysea Moresea, no students were ever on the school bus with Nichols after she was found to be drinking.
School administrators ensured all bus routes were covered.
Nichols is no longer employed by Greenup County Schools.
“Our number one goal is safety and we do not take reports lightly. We cannot and will not comment on the incident beyond the facts. At no point did students interact with the driver while they were impaired, and they did not ride with the driver while impaired. Thanks to the alertness of others, a scary situation had a safe ending. Please do not let this incident overshadow all the amazing drivers and staff members who serve at Greenup County Schools,” Moresea said in a statement.
Copyright 2024 WSAZ via Gray Media Group, Inc. All rights reserved.

Woman accused of shooting husband after catching him cheating on her, police say

50 Cent visits Shreveport to officially launch G-Unit Studios

NBA YoungBoy arrested in Utah on drug, weapons charges

Louisiana ranks no. 1 in U.S. for chlamydia cases, research shows

Louisiana’s first Buc-ee’s expected to open next year, bringing hundreds of jobs to the area
Latest news.

Shreveport welcomes 50 Cent with a party

50 Cent visits Shreveport to launch G-Unit Studios

Iran fires air defense batteries in provinces as sound of explosions heard near Isfahan

Beloved teacher couldn’t afford insulin, partially loses both legs, family says
Department News
Ph.d. student jaerim kim of professor haecheon choi’s lab claims the excellent research journal award in the 9th national congr.
- Next Master student Gahee Kwon of professor Yeon June Kang’s lab has claimed the Young Professional Grant in the I-INCE 2016
- Prev Professor Byeng Dong Youn’s Research Team Claims the Best Paper Award in QRQ2MSE 2015

Department of Mechanical Engineering
- Seoul National University
301-dong 116-ho, 1 Gwanak-ro, Gwanak-gu, Seoul 08826, Korea
Tel. +82-2-880-1911 | Fax. +82-2-888-6046 | Email [email protected]
- College of Engineering
- Multiscale Mechanics Design Major
- Institute of Advanced Machines Design
- Pahk's Creative Space
COPYRIGHT (C)2024 SEOUL NATIONAL UNIVERSITY. ALL RIGHTS RESERVED.
IMAGES
VIDEO
COMMENTS
Illicit drug use among teens has remained low and fairly steady for the past three decades, with some notable declines during the Covid-19 pandemic. In 2023, 29 percent of high school seniors ...
The short-term effects of alcohol consumption range from a decrease in anxiety and motor skills at lower doses to unconsciousness, anterograde amnesia, and central nervous system depression at higher doses. Cell membranes are highly permeable to alcohol, so once alcohol is in the bloodstream it can diffuse into nearly every cell in the body.. The concentration of alcohol in blood is measured ...
Nicotine is a naturally produced alkaloid in the nightshade family of plants (most predominantly in tobacco and Duboisia hopwoodii) and is widely used recreationally as a stimulant and anxiolytic.As a pharmaceutical drug, it is used for smoking cessation to relieve withdrawal symptoms. Nicotine acts as a receptor agonist at most nicotinic acetylcholine receptors (nAChRs), except at two ...
JEL Classification. There are no comments for this article. Peer Effects and Alcohol Use among College Students by Michael Kremer and Dan Levy. Published in volume 22, issue 3, pages 189-206 of Journal of Economic Perspectives, Summer 2008, Abstract: This paper examines the extent to which college students who drink alcohol influence their peers.
CEA simulations show that by 2055, a policy that increased the college going rate by 1, 3, and 5 percentage points could increase the level of GDP in 2055 (thirty years from now) by 0.2, 0.6, and ...
Despite the declining overall rate of cigarette smoking in the general population in the United States, the prevalence of smoking is estimated to be as high as 80% among treatment-seeking alcoholics. The serious adverse health effects of tobacco and heavy alcohol use are synergistic and recent evidence suggests that smoking slows the process of cognitive recovery following alcohol abstinence.
DOI: 10.29173/writingacrossuofa17 Corpus ID: 245629649; Effects of Positive Affirmation and Constructive Criticism on Student Writing and Success @article{Lunseth2021EffectsOP, title={Effects of Positive Affirmation and Constructive Criticism on Student Writing and Success}, author={Hayley Lunseth}, journal={Writing across the University of Alberta}, year={2021}, url={https://api ...
This study surveyed 115 undergraduate students at a largely commuter college in the suburban northeast. The data suggested that mental health issues increased since before the pandemic, while alcohol use has largely stayed the same over the course of the pandemic. Continued research in diverse college settings is needed on this important topic.
History and purpose. D.A.R.E. program materials from 1991 describe it as "a drug abuse prevention education program designed to equip elementary school children with skills for resisting peer pressure to experiment with tobacco, drugs, and alcohol." It was created as a part of the war on drugs in the United States, with the intention of reducing the demand for drugs through education that ...
Background: The high prevalence of cannabis use among young adults poses substantial global health concerns due to the associated acute and long-term health and psychosocial risks. Digital modalities, including websites, digital platforms, and mobile apps, have emerged as promising tools to enhance the accessibility and availability of evidence-based interventions for young adults for cannabis ...
This study investigated the impact of Omega-3 supplementation on social and academic outcomes in JSS III students with ADHD in Jigawa State. The cohort comprised predominantly male students (60%) with an average age of 14, attending mostly urban schools (70%). Results indicated a significant increase in social skills ratings from 2.5 to 4 out of 5, with 60% of students experiencing enhanced ...
The effects last for two to six hours, depending on the amount used. At high doses, mental effects can include anxiety, delusions (including ideas of reference), hallucinations, panic, paranoia, and psychosis. There is a strong relation between cannabis use and the risk of psychosis, though the direction of causality is debated.
GREENUP COUNTY, Ky. ( WSAZ /Gray News) - A school bus driver in Kentucky was charged Tuesday with public intoxication while she was waiting to take students home. According to a citation issued by the Flatwoods Police Department, Lisa Nichols, 57, was waiting for Greenup County students at an event. A staff member alerted police, and Nichols ...
Controversy. Opponents of drinking in public (such as religious organizations or governmental agencies) argue that it encourages overconsumption of alcohol and binge drinking, rowdiness and violence, and propose that people should instead drink at private businesses such as public houses, bars or clubs, where a bartender may prevent overconsumption and where rowdiness can be better controlled ...
Ph.D. student Jaerim Kim of professor Haecheon Choi's turbulence, flow control and CFD / Bio-Mimetic Engineering laboratory has claimed the Excellent paper award with the research titled "Effects of stenosis geometries on the pressure drop in coronary arteries" in the 9th National Congress on Fluids Engineering (9NCFE) held in the Daegu EXCO on 10th to 12th of August 2016.
Binge drinking, or heavy episodic drinking, is drinking alcoholic beverages with an intention of becoming intoxicated by heavy consumption of alcohol over a short period of time, but definitions vary considerably.. Binge drinking is a style of drinking that is popular in several countries worldwide, and overlaps somewhat with social drinking since it is often done in groups.
Cheese, like this Brie de Meaux, is high in saturated fats, and is a popular food in French cuisine.. The French paradox is an apparently paradoxical epidemiological observation that French people have a relatively low incidence of coronary heart disease (CHD), while having a diet relatively rich in saturated fats, in apparent contradiction to the widely held belief that the high consumption ...